
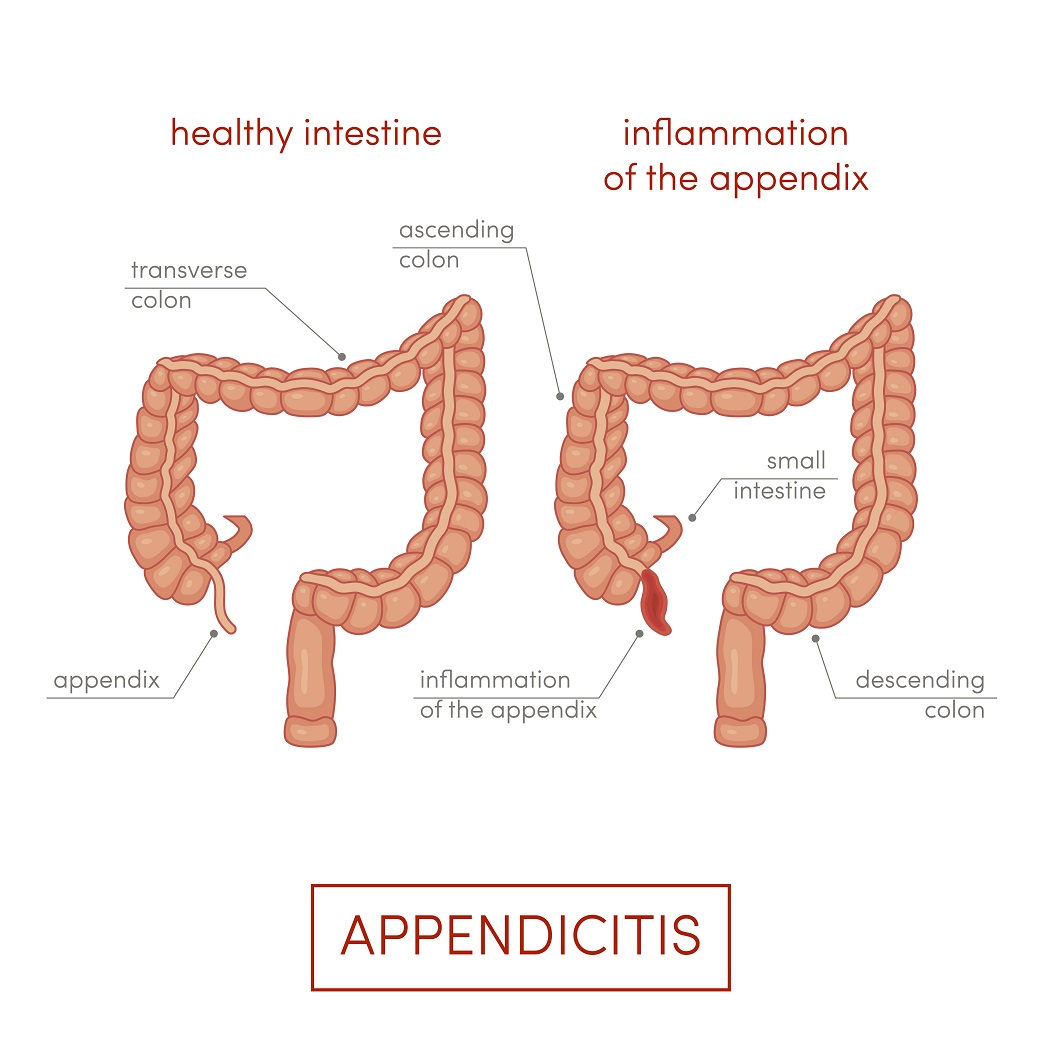
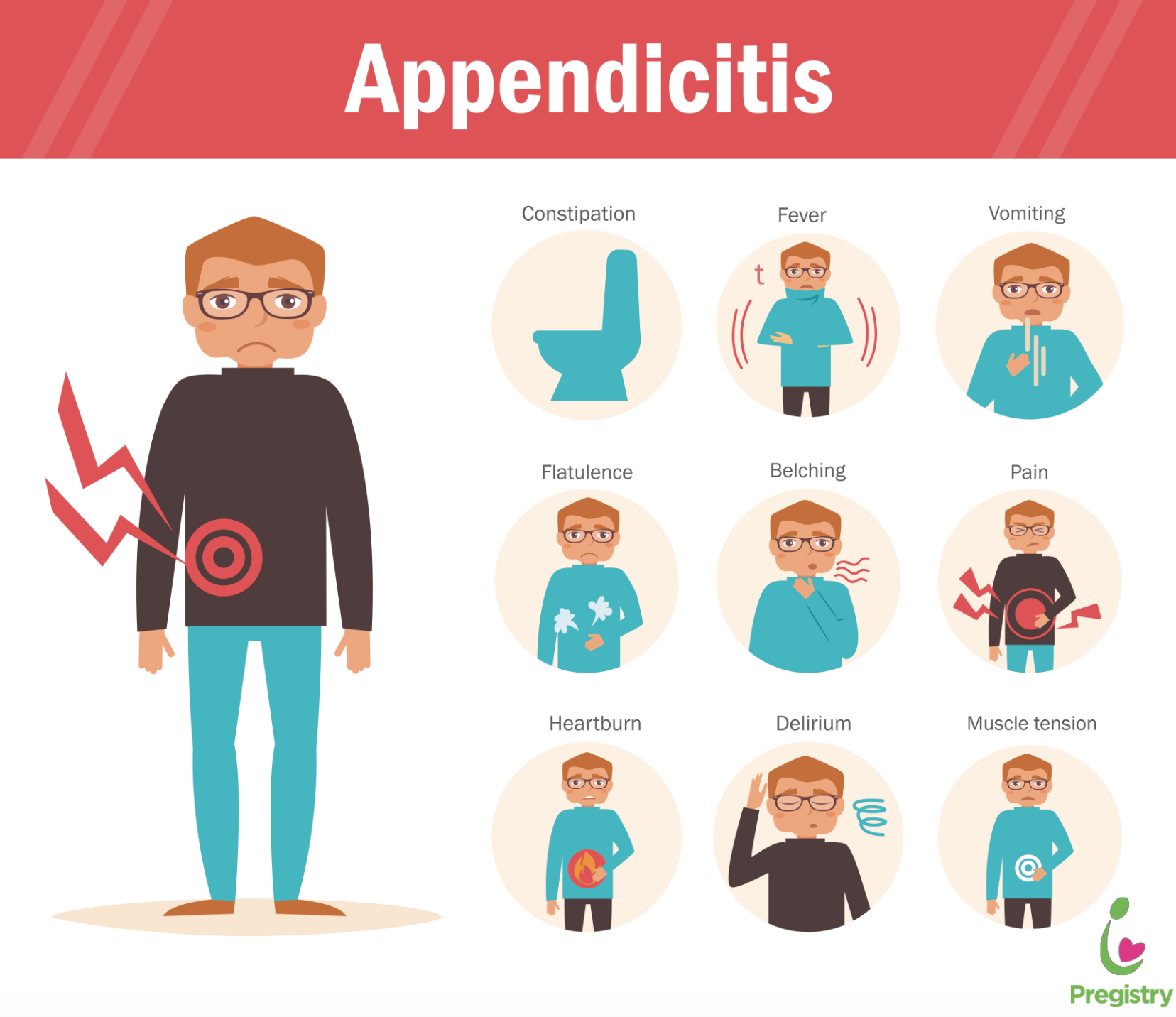
You may have heard of appendicitis, or you may know somebody who has had it. Usually when people say appendicitis, they mean acute appendicitis, which classically has been a surgical emergency, meaning that the affected person requires surgery immediately. Appendicitis means inflammation of the vermiform appendix, a sac-like appendage of the colon (the large intestine). Symptoms of acute appendicitis include abdominal pain. In non-pregnant patients, the pain typically begins gradually around the navel (dull, periumbilical pain) and over a period of 12-48 hours moves to the right side of the lower abdomen, but pain is often less severe when appendicitis occurs during pregnancy. Also, the location and movement of the pain can be very different during pregnancy since the pressure from the growing womb pushes the appendix into different areas of the abdomen. In particular, growth of the uterus shuffles the internal organs, pushing the appendix upward, toward the end of the second trimester so appendicitis pain is often in the upper right part of the abdomen during pregnancy. Along with modifying the pain during pregnancy, the relocation of internal organs also changes the usual signs that surgeons can expect to find when examining the abdomen for possible appendicitis. Apart from pain, symptoms of appendicitis also include nausea, anorexia (lack of appetite), vomiting, fever, increase in urination, and painful urination.
Standard treatment for acute appendicitis is removal of the appendix. The procedure is called an appendectomy, a very routine and safe operation when there are no other health issues and when appendicitis is detected early. However, appendicitis is a surgical emergency, and pregnancy can make the condition difficult to recognize. After all, the main symptom of appendicitis is pain and discomfort in the lower abdomen, and this is something that pregnancy can mask. Particularly during early pregnancy, women also can experience nausea and vomiting, which also are symptoms of appendicitis. Although fever is a classic symptom of appendicitis, pregnant women with appendicitis often lack a fever, so fever is not a very useful way to determine whether a pregnant woman has appendicitis.
In assessing patients for possible appendicitis, doctors will order blood tests to see if the number of white blood cells in the blood is elevated. This test is not so useful for diagnosis of appendicitis during pregnancy since the white blood cell count typically rises in pregnant women anyway. Therefore, what usually leads to a diagnosis of appendicitis in pregnancy is ultrasound examination, revealing that the appendix is swollen. If the ultrasound imaging does not give a clear result, doctors will order magnetic resonance imaging (MRI) of the abdomen to get a better look inside. It is very important to get the diagnosis correct for two reasons. First, missing appendicitis is extremely dangerous because if a perforated appendix develops, the lives of both the mother and the fetus will be in danger. On the other hand, if appendicitis is diagnosed falsely, then surgery will be performed for nothing, which will put the fetus at unnecessary risk.
Appendectomy has been the standard treatment for acute appendicitis for a very long time. Although there are records of appendectomies being performed as early as the 18th century, it was not until the very end of the 19th century that surgeons began performing appendectomies routinely as a way to prevent death of a patient that would result if a swollen appendix perforates, causing a very serious condition called peritonitis. The end of the 19th century through the early 20th century was the formative era of modern surgery, the time of surgical pioneers such as William Stewart Halsted who invented basic practices of surgery that enable operations deep in the body without major blood loss or infection.
For more than 100 years, doctors have assumed that if a patient is suffering from acute appendicitis, the appendix must simply be removed, preferably within 24 hours of when the severe pain, nausea, and other symptoms have begun. This is different from a related condition known as chronic appendicitis, in which the symptoms are more mild and often subside for long periods of time so it has not been considered a surgical emergency.
Appendectomy is a very routine and safe operation when there are no other health issues and when appendicitis is detected early. However, appendicitis is a surgical emergency, and pregnancy can make the condition difficult to recognize.
In recent years, doctors have demonstrated that uncomplicated cases of acute appendicitis–cases in which the appendix is swollen but not perforated–can be treated safely with antibiotic medications. When these medications are given correctly and early enough, in most cases the appendicitis will subside, and the patient will not require surgery. Now, because one of the last things that you want to have to do during pregnancy is surgery inside the lower abdomen, near the growing womb itself, the idea of treating uncomplicated appendicitis with medications instead of surgery sounds appealing. Unfortunately, research suggests that non-surgical treatment does not work as well for appendicitis occurring during pregnancy as it does for appendicitis in non-pregnant patients. Consequently, surgery is the standard treatment; however, the strategy as to which surgical technique to use, how to approach the appendix, and when to perform the operation depends on how advanced the pregnancy is. In some cases, the baby may need to be delivered before the appendix is removed.
Although it is unlikely that you will be given antibiotic treatment as a replacement for surgery if you have acute appendicitis while pregnant, there is another role for antibiotics, namely to prevent infection when you do have surgery. Although antibiotics given around the time of surgery must be selected based on their ability to protect against infections of the major groups of disease-causing bacteria—Gram-negative and Gram-positive bacteria and both aerobic bacteria (bacteria that breathe oxygen) and anaerobic bacteria (bacterial that do not breathe oxygen)—several antibiotics are fairly safe to give during pregnancy. Generally, pregnant women getting appendectomies are given metronidazole or clindamycin plus a drug from a family of antibiotics called cephalosporins.