Previously, The Pulse blogger Valerie DeBenedette wrote an excellent review on a common problem for boys, the undescended testicle (read it here). Two recent reviews on this topic, published in the Archives of Medical Science and the Canadian Urological Association Journal, update important information on risk factors and management of this most common congenital deformity in baby boys.
Undescended testis (UDT) may affect up to eight percent of full term boys and about one-third of premature boys, making it the most common birth abnormality in boys. Despite how common UDT is, there has been a lot of disagreement on how and when to treat it. Over the last 10 years, researchers from around the world have been working on these questions. Organizations like the European Society for Pediatric Urology, the European Association of Urology, and the American Urological Association have now reached some agreement on how to manage UDT.
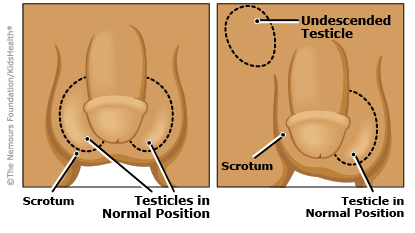
UDT Basics
Testicles form inside the belly and begin to migrate toward the scrotum at between 10 and 23 weeks of pregnancy. They may move into the scrotum through an opening called the inguinal canal, at around 34 weeks of pregnancy. A stimulus for this movement is the male hormone testosterone.
Testicles that don’t make it all the way down to the scrotum by birth get a second surge of testosterone at about age two to four months. This surge is called “mini puberty.” Because mini puberty may solve the problem, UDT should not be diagnosed before age six months.
UDT can occur on one side or on both sides. Unilateral UDT is four times more common than bilateral UDT. About 80 percent of UDTs can be felt (palpated) with a finger pressed high up into the inguinal canal. About 20 percent UDT’s are non-palpable. These testicles may be up inside the belly. If both testicles are non-palpable, there is a higher risk that there are no testicles. This is rare, but it may be a sign of a sexual differentiation disorder (an abnormality of the male or female sex chromosomes).
In some cases, the testicle or testicles are located near the inguinal canal but they can be pulled down (gently) into the scrotum. If this can be done, and the testicle stays in the scrotum for a minute or two, it is not a true UDT. This condition, called a retractile testicle, is caused by an overactive muscle (cremaster muscle). Exposure to cold or stress may trigger the muscle to retract the testicle (cremasteric reflex).
Risk Factors for UDT
The exact cause of UDT is still not known. Risk factors have been identified. These include:
- Premature birth (the most common risk factor)
- Low birth weight
- Small birth size
- A first or second pregnancy
- Having a difficult birth
- Using assistive reproductive technology (ART) to become pregnant
- Needing a C-section
- Having high blood pressure during pregnancy (toxemia)
- Nicotine exposure during pregnancy
- Diabetes during pregnancy
- A family history of UDT (father or sibling)
Treatment Guidelines for UDT
A physical exam with palpation is the best way to diagnose UDT. A soundwave (ultrasound) imaging study can be used to look for a testicle that cannot be palpated. The most important guideline for UDT is to have surgical correction (orchiopexy) before age 18 months. Early surgery reduces the three big risks of UDT. These risks are infertility, testicular cancer, and testicular trauma:
- A UDT is exposed to more body heat than a testicle that is down inside the scrotum. This few degrees difference in heat can prevent the testicle from forming normal germ cells that will become sperm cells. Studies show that an adult male with bilateral UDT has about a 60 to 65 percent chance of being infertile. Studies also show that the damage to germ cells may start in a UDT during the first 12 months of life. After age one, the loss of these cells may not be reversible. The testicle may shrink in size.
- The exposure to heat that causes germ cell damage may also increase the risk of testicular cancer in adult males. Ten percent of adult males diagnosed with testicular cancer have a history of UDT. The risk of testicular cancer may be 5 to 10 times higher than normal in these men. Orchiopexy before age 18 months may reduce this risk.
- A UDT has a higher risk for trauma. A testicle in the inguinal canal can be damaged by trauma to the groin area. UDTs are also at higher risk of losing their blood supply. This can be an emergency situation if a testicle twists around its blood vessels. This condition is called testicular torsion. Blood supply may be completely cut off and the testicle will die.
To prevent these complications, current guidelines say surgery should be done between 6 and 12 months, or by 18 months at the latest. In the 1970s, most orchiopexys were performed at around age five or six years. This may be too late to prevent damage. Studies show that most boys with UDT are still being treated too late.
Here is a summary of the current guidelines:
- UDT should not be diagnosed before age six months.
- A retractile testicle does not need treatment.
- If a child has bilateral, non-palpable UDTs, blood work should be done to rule out a sexual differentiation disorder before starting any treatment.
- Treating UDT with hormones to stimulate minipuberty should be avoided. This treatment was common in the past, but the success rate is very low, about 20 percent compared to success rates for surgery of 75 to 95 percent. There is a significant risk of testicular shrinkage from hormone treatment. Complications from surgery are low, about one percent.
- Palpable UDT should be treated through an inguinal incision. The testicle can be placed back in the scrotum in one procedure.
- A non-palpable UDT should be treated with laparoscopic surgery. This involves placing an operating telescope into the belly though a small incision. If the testicle is found inside the abdomen, the best way to fix it is with a two-stage surgical procedure called the Fowler-Stephens procedure. In the first step, short blood vessels attached to the testicle are removed. The second step is delayed so that the testicle can adapt to blood supplied by longer blood vessels. During the second procedure, the testicle can be placed into the scrotum.
- A UDT diagnosed after puberty should not be moved. It should be removed (orchiectomy) to prevent complications.
If you have a child diagnosed with UDT, the key takeaway from these guidelines is to make sure your child has surgery as early as possible after six months. The earlier the surgery, the better chance your child will have of avoiding complications from UDT.