
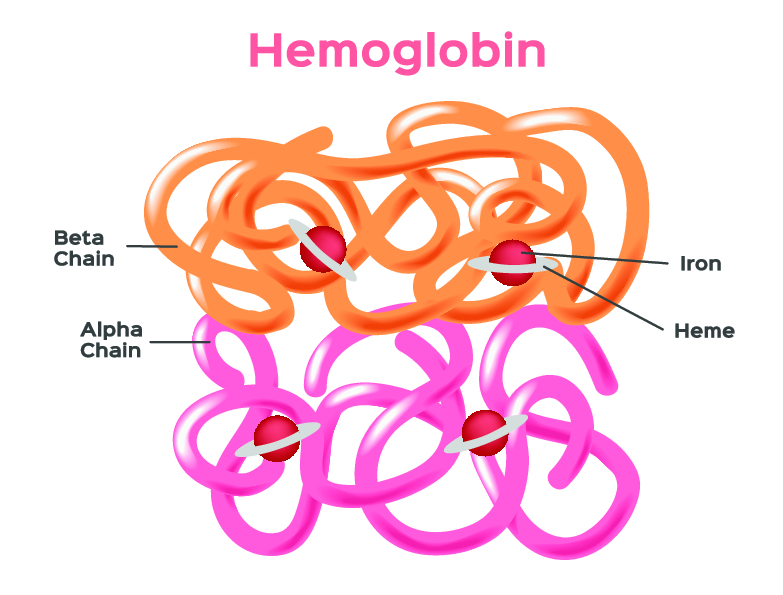
If a genetic condition called thalassemia runs in your family, there are several potential issues that you’ll need to consider along the pathway related to family planning and genetic counseling, to giving birth, and to raising your child. We’ll touch on those issues in the context of an overview of this condition. Thalassemia is a group of genetic diseases affecting red blood cells (RBCs) due to a problem in the production of hemoglobin, the oxygen-carrying molecule that fills each RBC. Each molecule of hemoglobin consists of four chemical entities called heme groups, each with an iron atom at its center that allows it to grab and release a molecule of oxygen (O2) and four protein chains called globins (see image below).
The genetics of thalassemia
In contrast with sickle cell anemia and certain other hemoglobin conditions in which the problem is production of a defective hemoglobin chain (in other words a qualitative problem), thalassemia is a quantitative problem with a hemoglobin chain. The genetics underlying both alpha and beta thalassemia is very complex, but there are a couple of points worth mentioning. The first is that most people carry two copies of the beta globin gene (one received from each parent) and four copies of the alpha globin gene (two from each parent). The other point is that most cases beta thalassemia result the presence of defects in one or both of the beta globin genes, whereas alpha thalassemia usually results from one or more of the alpha globin genes being absent. In cases when just one of the four alpha globin genes is absent, you would experience no symptoms and the condition is barely noticeable, even in standard blood tests (although it is easily detectable in genetic testing). On the other extreme, if a fetus is missing all four alpha globin genes, the condition is fatal and so health issues come into play during childhood and adult life, when two or three alpha genes are missing.
The severity of thalassemia
In the case of beta thalassemia, generally you may be affected minimally, if at least one of your two beta globin genes is normal. However, the situation varies since there are different types of defects that can exist in a beta globin gene, some causing a complete lack of production of beta globin from the affected copy of the gene but others causing reduced production. When both copies of the beta globin gene are abnormal, the severity of the beta thalassemia can vary substantially, depending on whether one or both gene copies are of the low-production or no-production type. Additionally, the severity of beta thalassemia is affected by the degree to which your blood cells have continued to make the fetal equivalent of beta chains, known as gamma chains.
As for the consequences of having thalassemia for pregnancy, this depends on the severity of your condition. With mild forms of thalassemia, pregnancy can trigger anemia, which may be partly due to iron deficiency related to pregnancy and partly from the thalassemia itself.
The classification of thalassemia
As a result of the various differences in chain production and resulting symptom severity, both alpha and beta thalassemia are classified as being minor or major plus there are various intermediate scenarios. You also may hear the term alpha or beta thalassemia trait. This means that you have minimal or no symptoms, but you are a carrier for a genetic makeup that can lead to thalassemia in your children. For instance, if you have one defective beta globin gene that gives you beta thalassemia minor, there is a 50 percent chance of passing that gene to your child each time you conceive. If the child receives the gene, he or she would be a carrier and could experience mild symptoms. However, if the child also receives a defective copy of the beta globin gene from her father, then she could end up with beta thalassemia major, a much more severe condition that includes frequent anemia and a frequent need for transfusion of donated RBCs.
Epidemiology of thalassemia
Thalassemia is fairly common, but your chances of having it depend greatly on your ancestry. Alpha thalassemia is most common in populations of Africa, Southeast Asia, Central America, the Mediterranean, and Middle East. Beta thalassemia also can occur in populations of the Mediterranean, Africa, and Southeast Asia, and also India, but it is particularly common in Greece, Italy, Coastal Turkey, Cyprus, and Sardinia. Thus, women who are mothers to be or who are planning motherhood and have Mediterranean roots should be tested for beta thalassemia and should receive genetic counseling.
Thalassemia in pregnancy
As for the consequences of having thalassemia for pregnancy, this depends on the severity of your condition. With mild forms of thalassemia, pregnancy can trigger anemia, which may be partly due to iron deficiency related to pregnancy and partly from the thalassemia itself. With an intermediate form of thalassemia you may experience some complications, but usually these can be managed by your obstetrician along with a blood specialist called a hematologist. With still more severe thalassemia, such as beta thalassemia major, successful pregnancy may be difficult as complications can be significant and tend to increase as quantities of iron build up in organs as a result of transfusions of RBCs given as treatment for anemia. In some women with beta thalassemia major, the spleen may grow to be very large and may need to be removed surgically, which increases the risk of infections and blood clots. Anemia also can be severe, require blood transfusions, and combined with the stresses of pregnancy may lead to heart failure.