Note: The Pregistry website includes expert reports on more than 2000 medications, 300 diseases, and 150 common exposures during pregnancy and lactation. For the topic Pneumothorax, go here. These expert reports are free of charge and can be saved and shared.
__________________________________
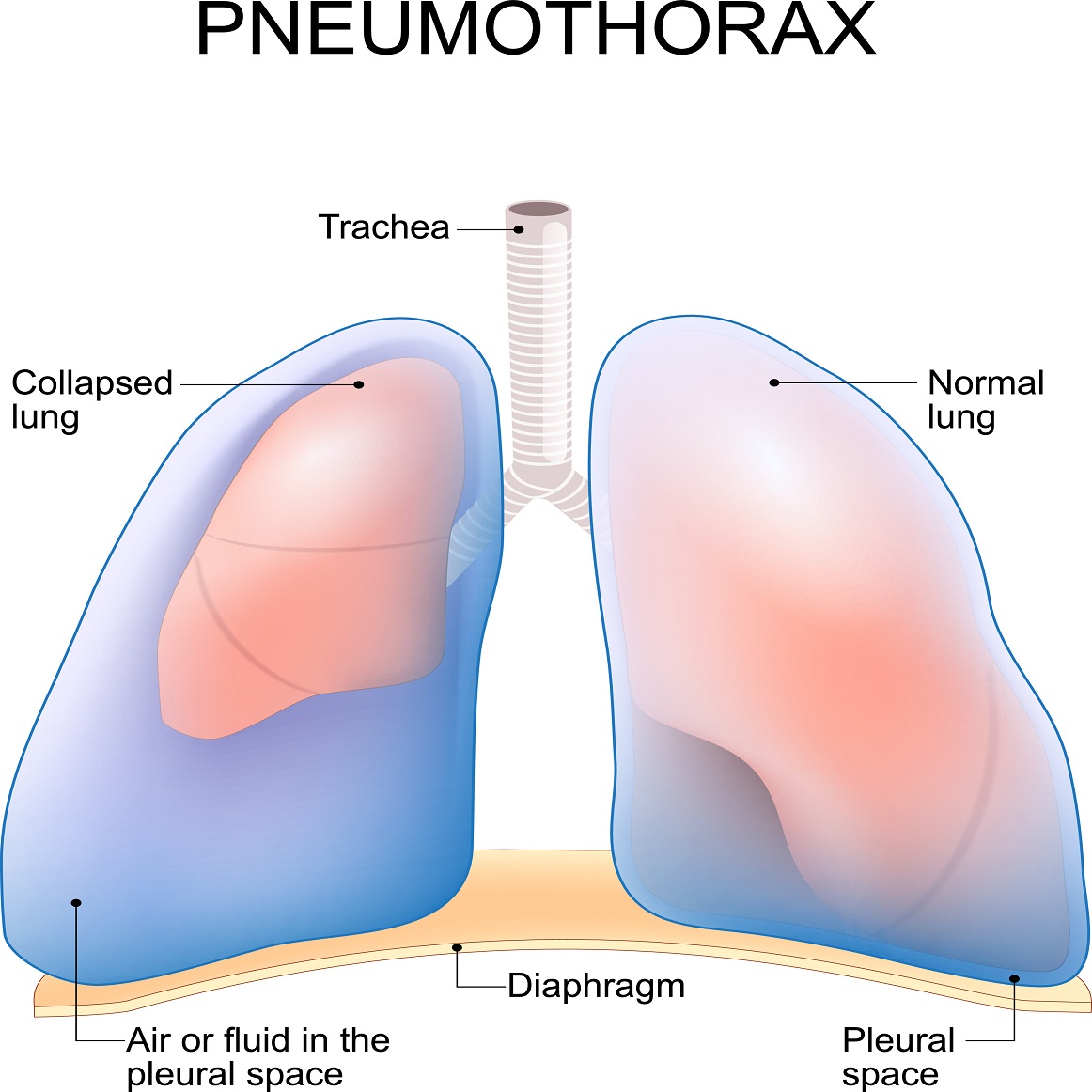
A pneumothorax (PTX) is a situation in which gas, usually air, enters the pleural space (also called the intrapleural space). This is a potential space between the membrane that covers the outside of the lungs and the membrane that covers the inside of the chest wall. Normally, the intrapleural space contains only a small amount of fluid that helps the membranes glide over one another. Also normally, the intrapleural pressure (the pressure in the intrapleural space) is just slightly lower than the atmospheric pressure outside the chest and in the lungs. The pressure difference enables the lungs to expand like balloons when you inhale, making the chest cavity larger. The expansion of the lungs draws in air. In a PTX, the intrapleural pressure rises within one side of the chest cavity due to a leak, either through the lung or through the wall of the chest cavity, which can be in the chest, the side, or the back.
In such cases, expansion of the chest to allow inhalation brings the intrapleural pressure closer to the pressure of the outside air and of the inside of the lung, making it difficult for the lung to inflate. Consequently, the lung collapses. Small holes can close without treatment, and the intrapleural pressure will gradually return to normal, but holes also can remain open, making breathing difficult because the lung on the affected side will be completely collapsed, or will inflate only slightly. Even so, as long as air can move back and forth through the hole, the other lung will continue to work. On the other hand, some injuries can act as a one-way valve, such that each time the person inhales, the intrapleural pressure on the affected side rises, yet does not decrease during exhalation. This can happen particularly with traumatic injuries through the chest, side, or back wall, and with broken ribs, but any type of PTX potentially can cause tension. In any case, a tension PTX is an extreme emergency, requiring immediate treatment, because the rising pressure can stop blood from returning to the heart and also can collapse the other lung.
Additionally, women, whether pregnant or not, can suffer what is called a spontaneous PTX, meaning a PTX that occurs without a traumatic cause or an obvious disease cause.
PTX can result from injury to the chest, including during cardiopulmonary resuscitation (CPR), from lung disease, or as a complication of mechanical ventilation. It also can result from pulmonary barotrauma, lung injury resulting from a sudden change in pressure that causes the lungs to expand too much. This can happen, if you’re holding your breath when the cabin suddenly depressurizes, or if you’re holding your breath while ascending during SCUBA diving. It also can happen to a victim of an explosion. Pregnant women should not SCUBA dive but otherwise PTX can occur during pregnancy for any of the reasons mentioned above. Additionally, women, whether pregnant or not, can suffer what is called a spontaneous PTX, meaning a PTX that occurs without a traumatic cause or an obvious disease cause. Relevant to non-pregnant women of reproductive age is another type of PTX called catamenial PTX (CTM), which is a PTX occurring in connection with menstruation.
PTX is largely a clinical diagnosis, meaning that it is diagnosed based on symptoms –notably breathing difficulty– and findings on the physical examination, notably absent breathing sounds on the affected side. Diagnosis can be aided by chest X-ray, which shows telltale signs, such as the absence of lung markings on the affected side. In the case of tension PTX, there is no time for imaging, so the diagnosis must be entirely clinical. In such cases, physical examination reveals not only absent breathing sounds, but the breathing is typically getting more difficult with each breath. Due to the pressure increasing on the affected side, it is often possible to see or feel the trachea (the “windpipe”) deviated toward the unaffected side.

PTX is treated with thoracostomy, in which an incision is made through the affected side of the chest, a tube is inserted through the incision, and attached to a kind of suction machine that restores the negative pressure over several hours. In the extreme emergency of a tension PTX, a thoracostomy can be made quickly with a needle, sheathed in a catheter (flexible tube), followed by removal of the needle with the catheter staying inside. This vents the pressure that has been rising, removing the immediate life-threatening danger, but a chest tube is then needed restore the negative pressure.
In the event that you suffer repeated pneumothoraces, subsequent to your pregnancy, you can be treated with a procedure called pleurodesis in which the lung on the affected side of the chest is fused of the inside of the chest wall, usually using some kind of chemical agent.