As noted in Part 1 of this multiple gestation series, we’re focusing on twins, because it’s the most common multiple gestation scenario and also because understanding the concepts related to twins helps with the understanding of higher order pregnancies. Genetically, there are two main categories of twins, the more common of which is called dizygotic twins. This means twins, each derived from its own zygote, its own egg that has been fertilized by a sperm. Genetically, such twins are like other siblings from the same pair of parents, meaning that they are not identical and can be either the same sex or one can be a boy and the other a girl. Known colloquially as fraternal twins, this is the more common situation, both in natural twinning and in twinning resulting from fertility treatment. Additionally, there are some unusual variations on dizygotic twins that we’ll discuss later in the this series, in Part 4, so let’s look now at the other main category, monozygotic twins.
Monozygotic twins are genetically identical, so they look alike and are always the same sex. Usually one zygote produces just one individual, leading to a singleton pregnancy. However, during the early days of cell division, the product of the zygote, the early embryo, can spit up into two, producing monozygotic twins. Occasionally, there can be splitting into more than two embryos, so there can be monozygotic triplets —identical triplets— as well as monozygotic higher numbers of siblings. We should also note at this time that in higher order pregnancies (triplets and higher), various combinations of monozygosity and multi zygosity are possible. Two or more of the babies can come from the same zygote and one or more of the others from different zygotes, so a mother can give birth to a litter of babies, some identical and some not.
But things get complex, depending on when the early embryo divides. Once a zygote forms from the fusion of the father’s chromosomes from a sperm cell with the mother’s chromosomes in the ovum, the zygote begins to cleave. Over a few days, it cleaves into two cells, four cells, eight cells, and so forth. This leads to a ball of identical cells, called a morula, but then the cells of the morula start to differentiate, meaning some cells act differently from other cells. Over the course of a few more days, the morula becomes a blastocyst. This is the type of early embryo that implants into the lining of the uterus (the endometrium), which can happen naturally several days after sexual intercourse, or as a result of embryo transfer (ET), in which early embryos created by way of in vitro fertilization (IVF) are injected into the uterus as fertility treatment. In contrast with a morula, a blastocyst consists of parts that are not all the same, because cells have begun to differentiate. At one end, a cavity of fluid, called a blastocoel, while a concentration of cells called the embryoblast forms at the other end, thus on one side of the blastocoel.
Meanwhile, the outside of the embryoblast and most of the blastocoel are surrounded by a layer of cells, called the trophoblast. After implantation, the trophoblast will connect to the uterus and be the medium through which oxygen and nutrients reach the embryo from the mother’s blood and through which waste products move from the embryo to the mother’s blood. Most of a membrane, called the chorion, will arise from the trophoblast, and the chorion will give rise the placenta, the organ that will support the embryo and later the fetus.
As for the embryoblast, it will give rise to the embryo and gradually distinguishing itself from the trophoblast. The latter happens with the formation of the blastocoel on one side of the embryoblast, and soon after with the formation of another fluid-filled cavity, called the amniotic cavity, on the other side of the embryoblast. Separating the amniotic cavity from the chorion will be another membrane, a more inner membrane, called the amnion. For the fetus to pass through the birth canal, both the chorion and the amnion will need to rupture, an event that typically happens early in labor. Colloquially, that’s what people mean when the say that your water has broken, since rupturing of the membranes releases amniotic fluid.
Now if you have a dizygotic pregnancy, then all of these categories of cells and membranes have formed separately for each embryo. This leads to two fetuses, each surrounded by its own chorion and having its own placenta and its own amniotic sac, but when there’s a monozygotic pregnancy, various scenarios are possible.
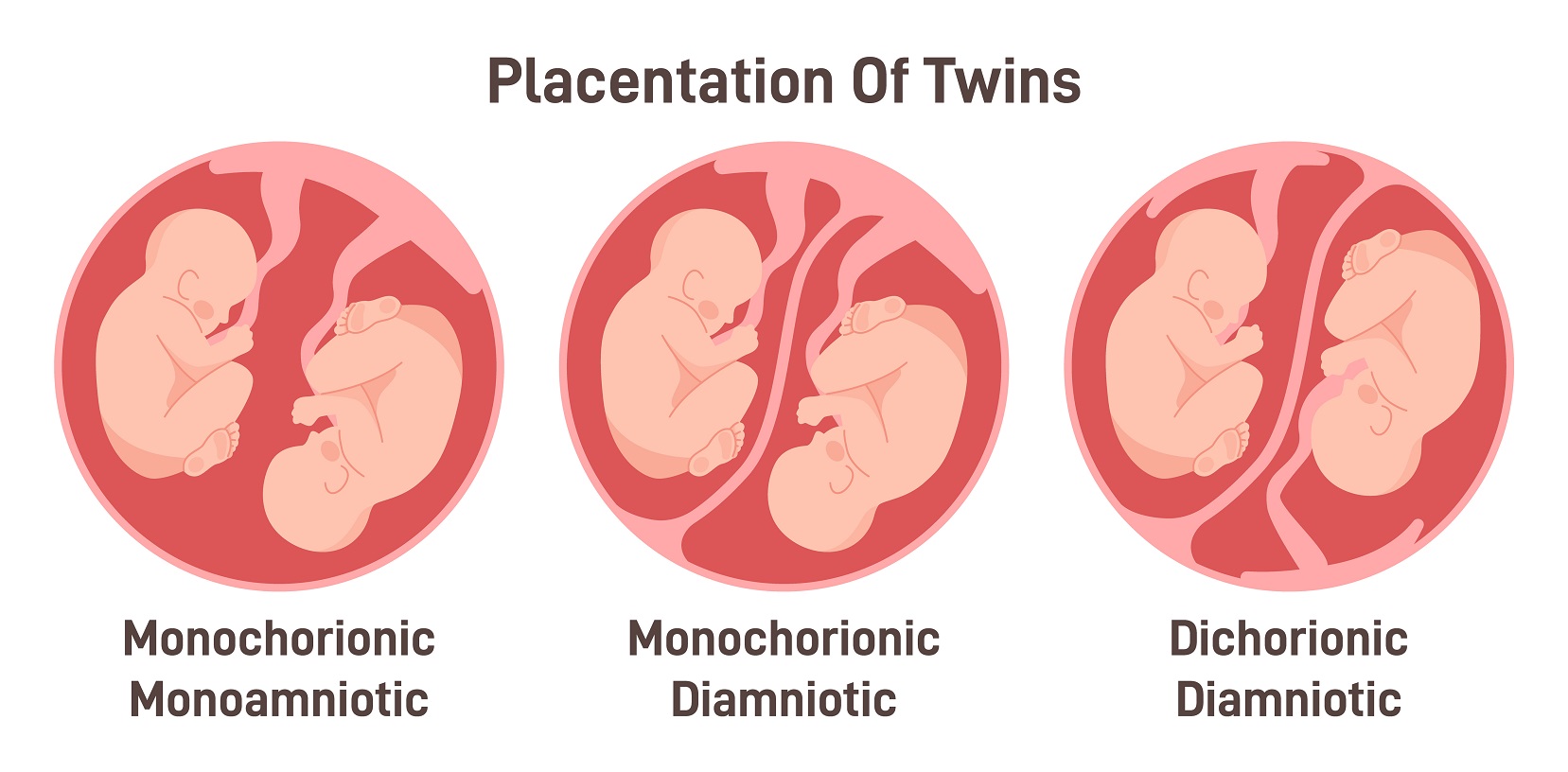
If the embryo splits into two while in a zygote stage (two cell, four cell, eight cell, etc) or as a morula —in other words during the first 3 days or so after fertilization— in terms of the membranes, the situation for the twins will be like that of dizygotic twins. Each will have its own placenta and its own private amniotic sac. This is called a dichorionic, diamniotic pregnancy. Everything is like that of a dizygotic pregnancy, except genetically the twins are identical (monozygotic).
If the split happens a little later, during the blastocyst stage, up to about day eight post-fertilization, this means that there already was a distinct trophoblast prior to splitting, so the two twins end up sharing a chorion, and thus sharing a placenta. But they each will get their own amnion, because the amnion forms a little bit after the time of the split. This is the most common type of monozygotic pregnancy and it’s called a monochorionic, diamniotic pregnancy. But what if the split happens even later? Well, if the embryo splits between days 8-13, it produces a monochorionic, monoamniotic pregnancy. This means that within that single chorion, there is only one amniotic sac. The twins are floating together with no physical separation. Finally, if the split happens days 13-15, some parts of the embryos themselves do not fully separate, so this produces conjoined twins. Fortunately, the latter case is extremely rare.
In Part 3, we’ll discuss these different types of twinning in terms of the clinical implications.