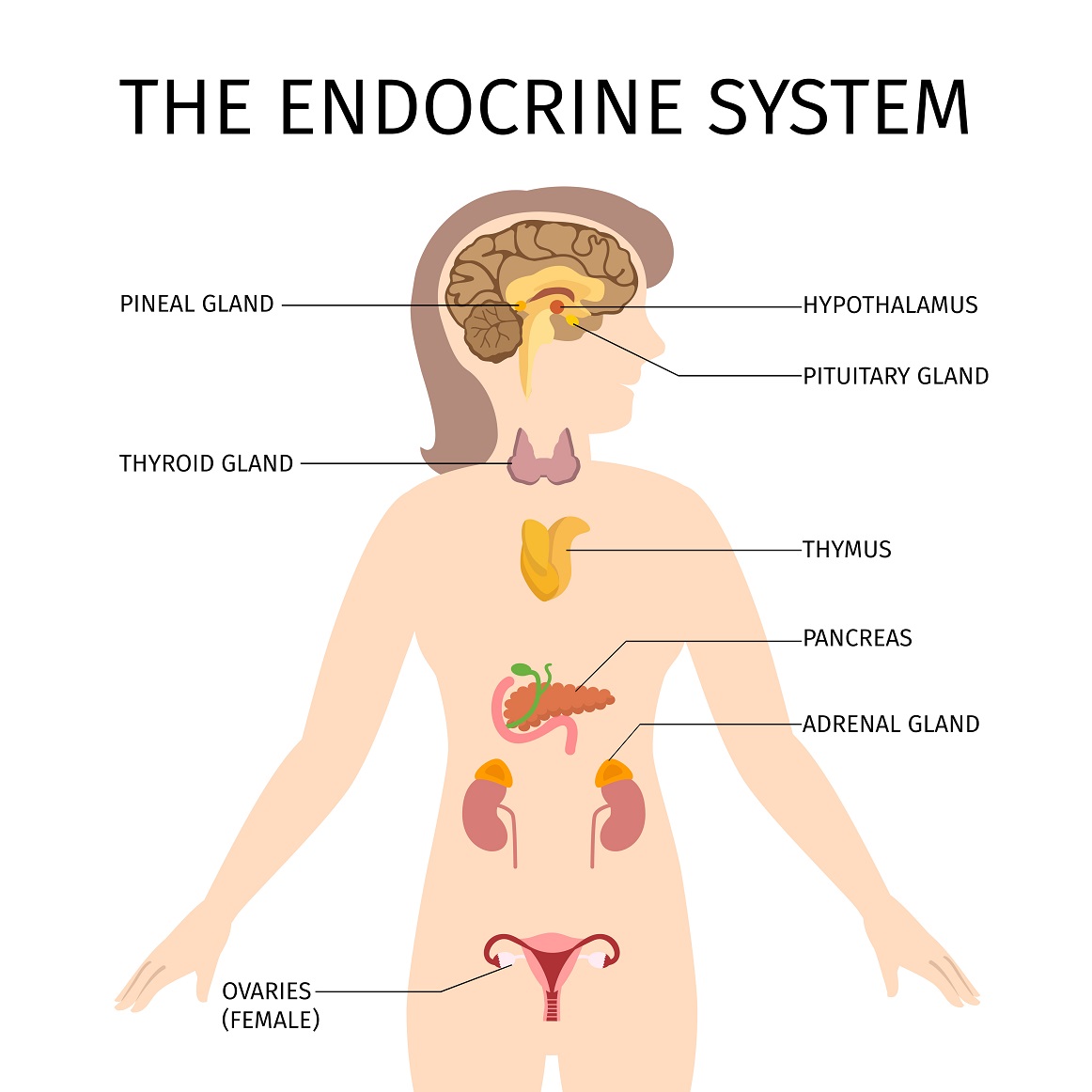
In previous installments of this series, we have looked at how pregnancy changes the physiology of body systems, such as the respiratory system, the circulatory system, the digestive system, and the urinary system. Today, we’ll discuss the endocrine system in terms of what changes during pregnancy. The endocrine system consists of glands that make hormones and secrete them into the blood. The endocrine glands consist of the hypothalamus and pituitary (both located in the brain), the thyroid and parathyroid glands (located in the neck), the adrenal glands, located on top of the kidneys), the pineal body (located in the brain), the ovaries in women, and the testes in men. As pregnancy advances through its early phases, a woman’s ovaries secrete in creating amounts of the hormones estrogen and progesterone. Initially, the progesterone is produced by a kind of temporary gland within the ovary called the corpus luteum, but later the placenta takes over, producing increasing amounts of both progesterone and estrogen. Through the first seven weeks of pregnancy, essentially all of the progesterone comes from the corpus luteum. From ten weeks onward, however, the placenta produces all of the progesterone. The period in between, from week 8 through week 10 is a transitional period that obstetricians call the luteal-placental shift, during which the placenta gradually takes over.
An important concept for you to know is that pregnancy is counted in terms of gestational weeks, whose starting point is the time of your last menstrual period. After that period, you need to ovulate, which typically takes 14 days, though with a lot of variation; some women take less time and some more. An ovum (egg) then needs to be fertilized, resulting in a zygote, which undergoes cell division, over and over, leading to an entity called a blastocyst by about five days after fertilization. For you to become pregnant, the blastocyst, essentially an early embryo, must implant into the endometrium, the inner lining of your uterus, which happens around five to six days after fertilization. This means that you are not actually pregnant until the third or the early fourth gestational week. For implantation of a blastocyst to occur, the endometrium must be prepared by exposure to progesterone. The needed progesterone comes from the corpus luteum. If something goes wrong with the corpus luteum prior to implantation, implantation will not occur, so there will be no pregnancy. Similarly, if something goes wrong with the corpus luteum prior to the placental production of progesterone getting started at eight weeks and then ramping up, the pregnancy will abort spontaneously. For the same reason, up to at least the end of the 10th gestational week, elective abortion can be induced, simply by administering a medication that blocks the actions of progesterone.
While the corpus luteum continues to produce progesterone until the placenta has formed and is ready to begin providing progesterone and other hormones, the implantation of a blastocyst triggers a process that starts producing another hormone, beta-human chorionic gonadotropin (β-hcg) from special cells and eventually from the placenta. β-hcg is the hormone whose presence is detected by pregnancy tests. Home pregnancy tests look for β-hcg in urine, while pregnancy tests that your doctor gives you check β-hcg levels usually in urine, but can also use a sample of blood. Meanwhile, two hormones from the pituitary that are very important to the ovarian cycle each month, luteinizing hormone (LH) and follicle-stimulating hormone (FSH), kind of drop off the radar screen during pregnancy, LH remaining at the low end of its normal range and FSH dropping much lower than it ever gets when you are not pregnant.
As the placenta grows and develops, increased quantities of progesterone and estrogen that it puts out stimulate the mother’s liver to increase its production of a protein called thyroid-binding globulin (TBG). TBG is one of a few proteins to which thyroid hormones, T3 and T4, can attach as they travel in the bloodstream and in other body fluids. Normally, these thyroid hormones are mostly bound to such proteins, but some amount of the hormones also exist freely in the blood. Based on the concentration of free (unbound) thyroid hormones, the hypothalamus, in the brain, decides whether, and to what degree, the production of thyroid hormones needs to be boosted —just like the thermostat in your house decides when to turn on the air conditioning or heating based on temperature measurements. Extra TBG from the liver means that less thyroid hormone is unbound, which fools the hypothalamus into thinking that there are lower concentrations than there actually are, so the hypothalamus sends out thyrotropin-releasing hormone (TRH) to the pituitary. The pituitary responds to the TRH by boosting its production of yet another hormone, thyroid stimulating hormone (TSH). This is the first hormone that doctors check if they think that you may have a thyroid problem, because it gives a better indication of whether the thyroid is under-or overactive than even the levels of thyroid hormones themselves provide. In pregnancy, however, the boosted TSH is a a product of the changes in the liver, but result of increased TSG, as when you are not pregnant, is that it stimulates the thyroid hormones, which are important, not only for you, but for the normal development of the fetus.
Endocrinology of pregnancy involves various changes in production and handling of various other hormones that have discussed. These include prolactin from the pituitary, placental lactogen from the placenta, and hormones that you may have heard about on non-pregnancy settings, such as cortisol from the adrenal glands, melatonin from the pineal, which helps with sleep, and insulin from the islet cells of the pancreas. They also include hormones that become particularly important during labor, notably oxytocin (from the hypothalamus), which makes your uterus contract, and epinephrine, which relaxes your uterus at the end of labor, but also has numerous effects on blood vessels. You may know that diabetes mellitus results from either inadequate production of insulin (type 1) or resistance (decreased ability to respond) to insulin (type 2). Normal pregnancy entails increased insulin resistance, which can make type 2 diabetes worse, but also can lead to gestational diabetes (diabetes that is particular to pregnancy).