Each year, a number of babies are born with a birth defect of the lips and mouth called a cleft lip or cleft palate. Cleft lip and cleft palate can occur together, but a baby can have either one or the other. These conditions can present problems in the care and feeding of a baby, but they can be corrected.
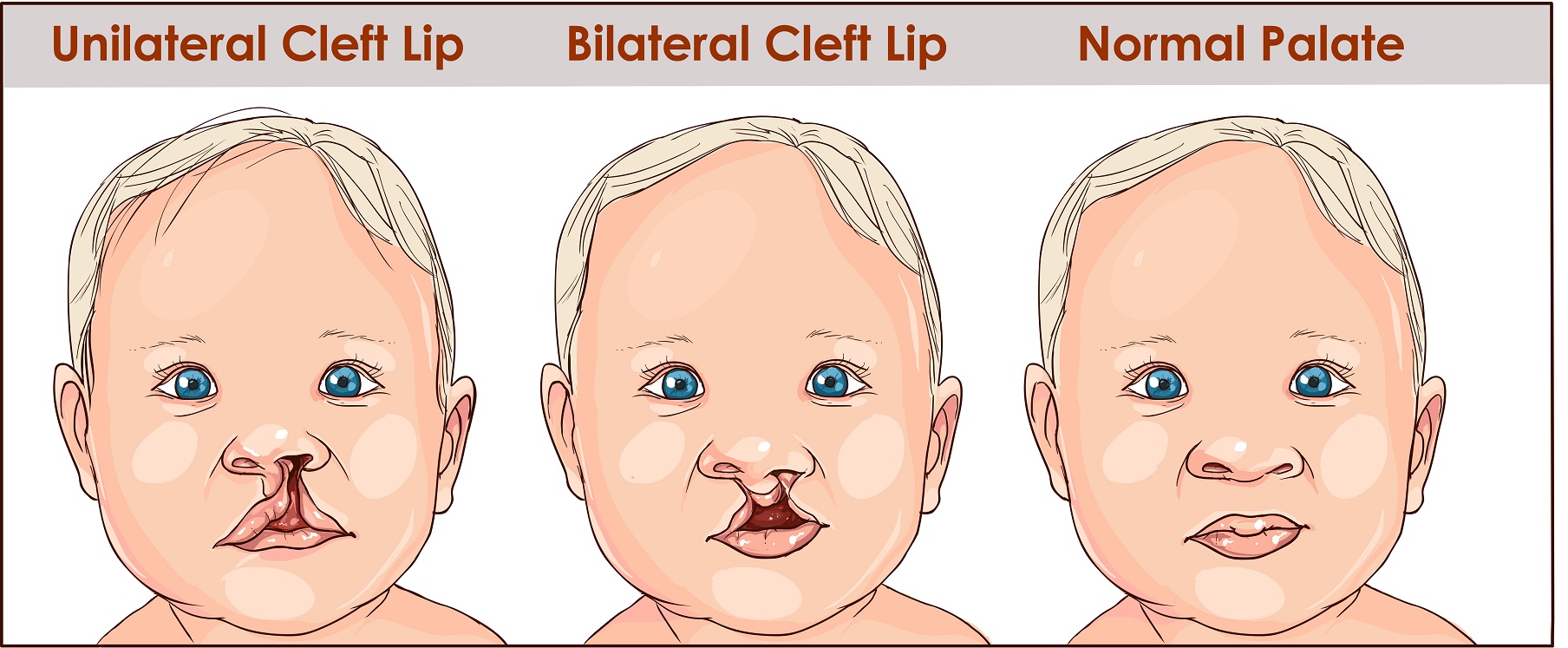
With a cleft lip, the baby has a split in the upper lip right under the nose. The split can be a small notch in the lip or can extend up into the nostril. The split will usually be on one side of the nose or the other, but there can be two splits that extend into the nostrils, which is called a bilateral split lip.
With a cleft palate, the roof of the mouth has not formed correctly and there is a gap or hole there that connects the mouth to the nasal passages behind the nose. As with a cleft lip, the hole may be small or large. When cleft palate is combined with cleft lip, the baby may also have malformations of the nose as well.
According to the Centers for Disease Control and Prevention, about one in every 1,600 babies is born with both cleft lip and palate, one in very 2,800 babies is born with cleft lip, and one in every 1,700 babies is born with cleft palate.
Both cleft lip and cleft palate occur because the formation of the central part of the face is interrupted early in the pregnancy. The face and mouth are formed when skin, bone, and cartilage grow from either side of the face toward the middle, where they unite to create a complete face. This formation happens during the first few weeks of a pregnancy.
These types of birth defects are also called orofacial or craniofacial defects.
The causes of cleft lip and palate are not completely known. However, it is known that women who smoke and those who have diabetes have an increased risk of having a baby with a cleft lip or palate. Women who binge drink alcohol also have an increased risk. Certain medications that are used to treat epilepsy and seizures also can raise the risk. Genetics also appears to play a role.
Getting enough of a nutrient called folic acid helps lower the risk of cleft lip and cleft palate. Most women don’t get enough folic acid in their diet and should take prenatal vitamins if they are planning to become pregnant. Because folic acid also helps reduce the risk of birth defects to the spine and head, it is added to enriched grains products like bread and pasta.
Birth defects of the lip and palate can sometimes be identified on an ultrasound before birth, but often they are only discovered when the baby is born.
Babies with cleft lip and palate, or both, can have issues with how their teeth grow in, problems in learning to speak, and problems with hearing. Cleft lip and palate can also be associated with birth defects elsewhere in the body.
A baby with a cleft lip or cleft palate, or both, may have difficulty with feeding properly. A baby with a cleft palate will need to be fed with special bottles. Because of the cleft in the palate the baby may not be able to form a suction around the nipple of the bottle. Some milk or formula may go up through the cleft and come out the nose. The baby may need to be held in an upright position while being fed so that formula or breast milk flows down to the throat. The baby may also swallow a lot of air during feeding and will need to be burped more often.
Even with bottle feeding, breast milk is best for the baby since it supplies the best nutrition and immune support. The mother can pump her breast milk to feed her baby.
Babies with a cleft lip who do not have a cleft palate can be breastfed successfully, but they may have trouble latching on.
This information about feeding is general advice. You may receive different instructions on the best ways to feed your baby. You should follow those instructions.
Soon after a baby with cleft lip or palate is born, he or she will be evaluated by a team of healthcare professionals to determine how extensive the cleft is. The team will create a treatment plan that is individualized to each baby. Team members include nurses, surgeons, audiologists, pediatric orthodontists and dentists, and speech pathologists.
Most babies with craniofacial defects have surgery to help correct the problem within the first year of life. Surgery will help with the function of the baby’s mouth, help allow for teeth to come in normally, and give a normal appearance. Usually, a cleft lip without a cleft palate will be repaired during the baby’s first few months. A cleft palate without a cleft lip can usually be corrected by the baby’s first birthday. Some babies with an extensive cleft or with combined cleft lip and cleft palate may need a series of surgeries as they grow.