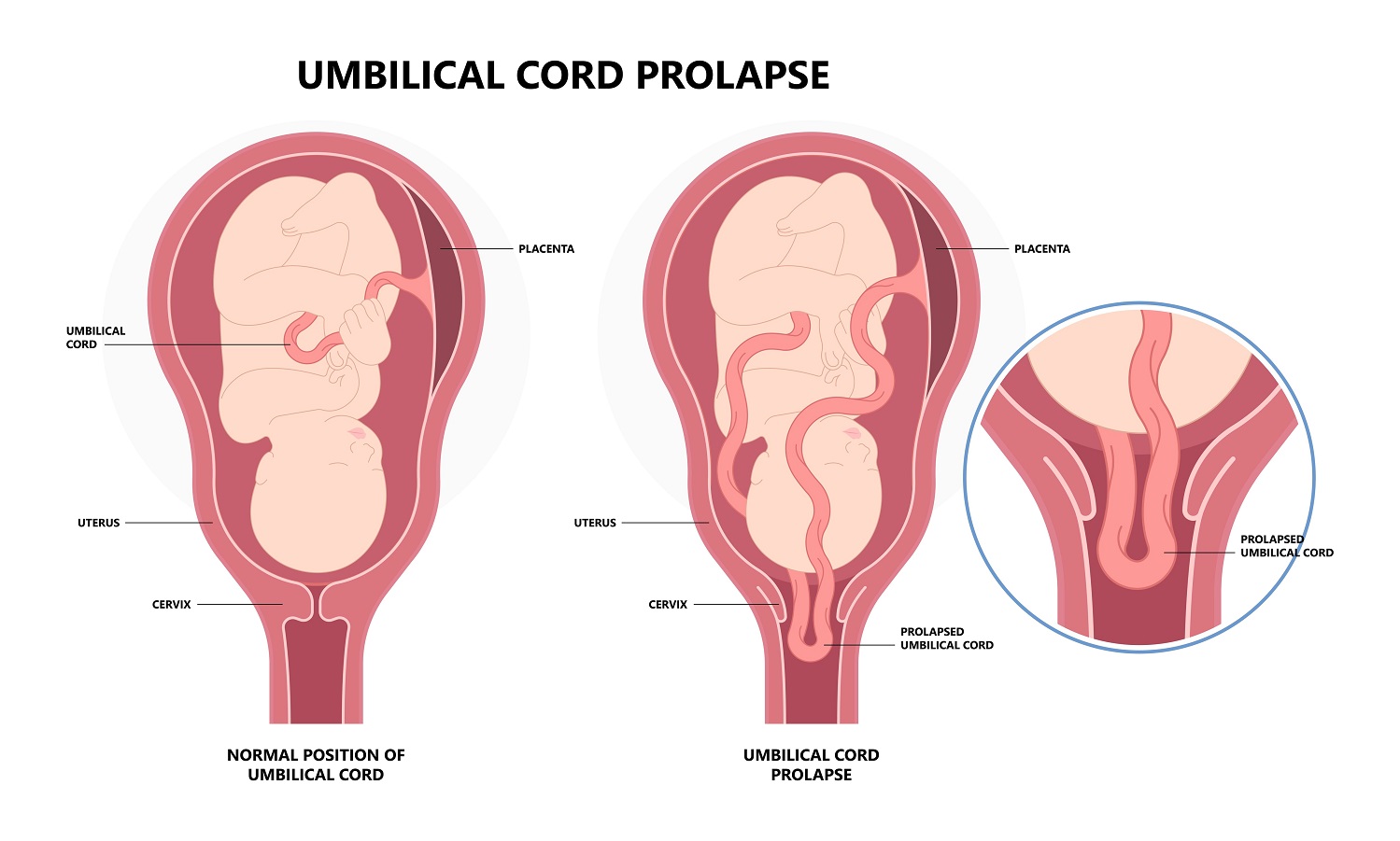
Umbilical cord prolapse is a condition in which the umbilical cord descends beneath the presenting part of the fetus. This means that the cord is below the head in a normal cephalic (head down) presentation and passes through the cervix into the vagina after rupture of the fetal membranes (water breaks). This compresses the umbilical cord, causing fetal hypoxia, meaning lack of oxygen to the fetus. The greatest risk factor for umbilical cold prolapse is a situation in which the fetus is in an abnormal lie after 37 weeks gestation. I’m not talking about a breech lie in which the fetal head is up, and the bottom or legs are facing down, but rather an unstable lie, such as transverse (the fetus is sideways in the womb) or oblique (the fetus is on an angle). These lies allow enough space and cord slack for the cord to prolapse through the cervix. In contrast, in a normal presentation, the head of the fetus moves quickly into the pelvis, so there’s no room for the cord to descend or prolapse. There is also usually not so much room for the cord to prolapse in cases of breech, so generally it’s the transverse and oblique presentations when this happens.
Doctors will suspect umbilical cord prolapse when cardiotocography (CTG), an ultrasound system that records the fetal heart rate shows signs of fetal distress. In cases like this, doctors can confirm presence of a prolapsed umbilical cord by way of a vaginal examination using a speculum.
Umbilical cord prolapse requires and emergency cesarean section. This is a surgical delivery in which the obstetrician cuts an incision through your abdomen, then through the muscles that comprise the bulk of the wall of the uterus where the fetus is developing. In most cases, the surgical approach for a cesarean will be through a low transverse incision, what most people know it as a ‘bikini cut’, since it runs horizontally around the same level where many bikinis reach. Usually, this type of incision is curved but there’s another type of transverse incision that is straight and a little bit higher up. If it’s an extreme emergency, it’s possible that the obstetrician will opt for a vertical incision instead. This could be a low vertical incision, which starts around the same level as a low transverse, but running up and down, instead of side to side. Also, there is a classical incision, which means vertical, but higher up the abdomen compared with the low vertical. The classical incision can be extended longer than the low vertical and gives the surgeon quick access to the womb, which could be critical in an extreme emergency.
Cesarean section is routine and very safe. Compared with vaginal birth, cesarean offers certain advantages, particularly for the baby. As with vaginal birth, you can be awake as your child enters the world, but you will still receive anesthesia, which will be either spinal anesthesia or epidural anesthesia. Both of these types of anesthesia prevent pain below a certain level on the body and both are induced through a needle that the anesthesiologists passes between two vertebrae in the lower spine. In the case of spinal anesthesia, a local anesthetic agent is injected through the layers of connective tissue that surround the spinal cord and into what’s called the subarachnoid space, where there is fluid, called cerebrospinal fluid. In the case of epidural anesthesia, the anesthesiologist does not advance the needle as deeply and injects the anesthetic on the surface of the most outer layer of connective tissue, called the dura mater.
Cesarean section is necessary in cases of umbilical cord prolapse because a normal vaginal delivery carries a high risk of putting pressure on the cord, cutting off blood flow and thus oxygen to the baby. In caring for a pregnant woman with umbilical cord prolapse, health care workers need to keep the cord warm and wet and minimize handling of the cord while waiting for delivery. Handling the cord puts pressure on it, which causes vasospasm, meaning that the blood vessels go through episodes of contraction. The cord squeeze up, keeping the blood from moving through. In cases when the fetus is compressing a prolapsed cord, the presenting part of the fetus, can be pushed up. This relieves pressure on the cord, allowing gravity to draw the fetus away from the pelvis and reduce compression on the cord. The patient can lie on her left side with a pillow under the head, or she can lie on all fours, in what is called the knee chest position. Doctors will give medications called tocolytics, which relax the uterus to reduce the fetal distress until the cesarean delivery can be performed.