We began our discussion of congenital heart disease here on The Pulse with a post about Tetralogy of Fallot and and another one about transposition of the great arteries. Today, we’ll take the discussion to a type of congenital heart disease called tricuspid atresia. Recall from our discussions of the cardiovascular system (circulatory system) and circulation in the fetus that that the tricuspid valve is one of four valves that regulate blood flow in the heart. Normally, the tricuspid valve controls the movement of blood from the right atrium (the right upper chamber) into the right ventricle (the right lower chamber). Before discussing tricuspid atresia, it’s important to review the normal pathway that blood takes through the body subsequent to birth, because the management of tricuspid atresia involves changing this pathway considerably.
Normally, after supplying body tissues with oxygen (O2), glucose (blood sugar), and other vital chemicals, and carrying away carbon dioxide CO2 and other waste products, blood arrives in the atrium. This is the point when the tricuspid valve becomes important, because blood in the right atrium moves through the tricuspid valve into the right ventricle. When the right ventricle contracts, pressure rises in the right atrium and the leaflets of the tricuspid valve close, preventing blood from flowing back into the right atrium, while the pulmonary valve opens, allowing blood into a large vessel, called the pulmonary artery. The pulmonary artery splits into left and right branches, each of which branches into an increasing number of vessels that carry blood through the left and right lungs, respectively. In special capillaries in the lungs’ air sacs, blood releases CO2, which is exhaled, and absorbs O2. The freshly oxygenated blood moves into a system of increasingly larger veins that converge into a few (usually four) pulmonary veins that deliver blood to the left atrium. When the ventricles relax, blood that’s in the left atrium begins moving through another valve called the mitral valve (also called the bicuspid valve) into the left ventricle. As that happens, the atrium contracts, providing an added kick to get more blood from the atrium into the ventricle. Then, when the ventricles contract, the mitral valve closes, pressure rises, and blood moves through the aortic valve, into a large vessel called the aorta. From the aorta, numerous arteries branch off, supplying body tissues, from which blood returns again to the right atrium, ready for another trip. Notice that there are really two circuits of blood flow, one pumped by the right ventricle sending blood through the lungs, the other pumped by the left ventricle, sending blood through the body.
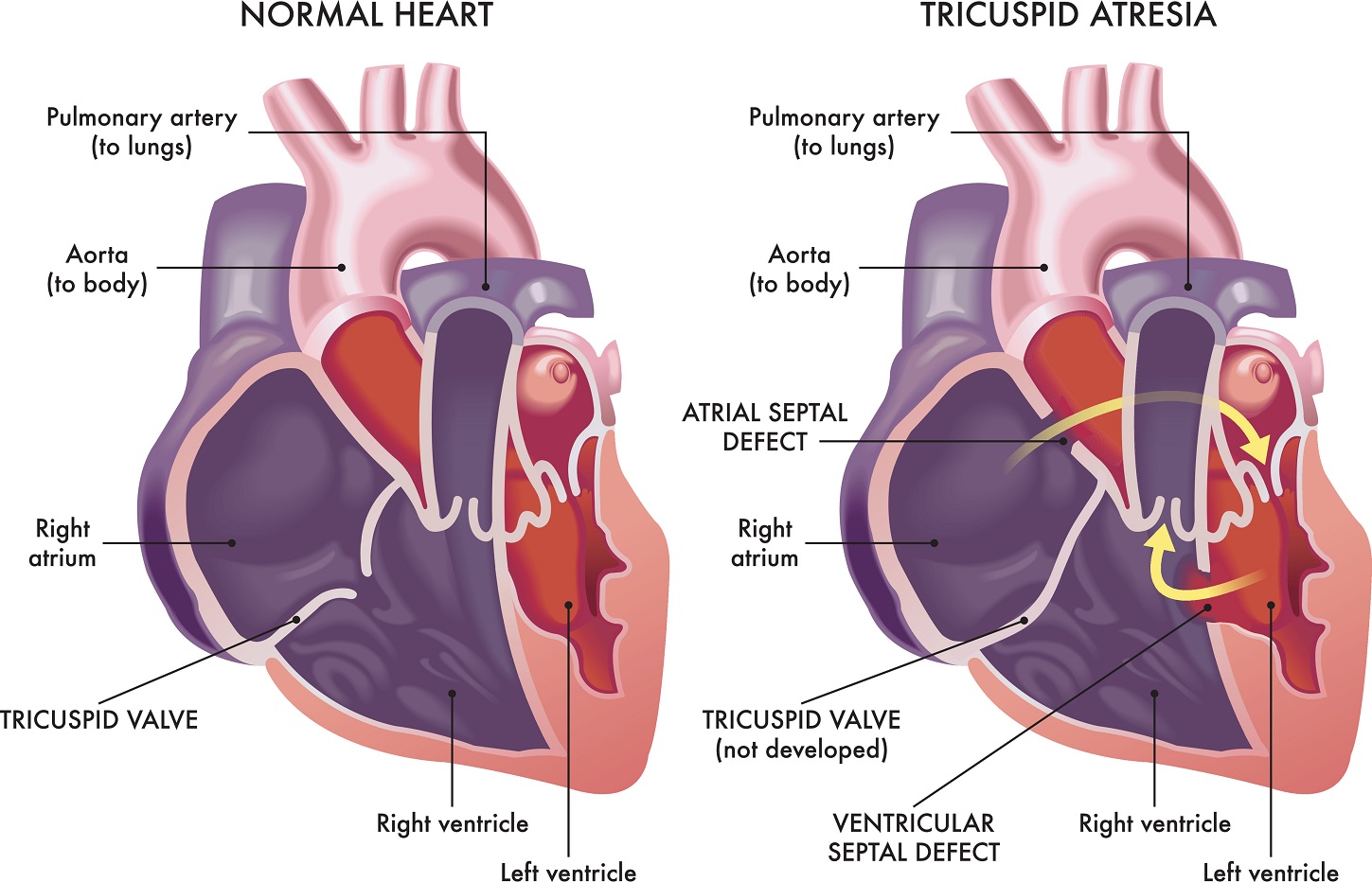
Atresia means that an opening that’s supposed to be there isn’t there. Instead of a valve, you have basically just a wall. If the tricuspid valve is atretic, there’s no way for blood to get from the right atrium into the right ventricle, at least not directly. The only way that the blood can go is through the foramen ovale, a passageway into the left atrium that’s present through fetal life. Alternatively, blood can go through an ASD —an atrial septal defect— meaning a hole in the wall that normally separates the two atria. Such a defect is common among babies born with the very uncommon condition of tricuspid atresia. There also can be a ventricular septal defect —VSD— a hole in the wall between the two ventricles, which is actually helpful in this case. One way or another, blood has to get into the left atrium, because there is no direct route into the right atrium.
Blood also has to get to the lungs and there are two ways that this can happen. One way is through the ductus arteriosus, a vessel connecting the aorta to the pulmonary artery. This is present throughout fetal life and, knowing that a baby will be born with tricuspid atresia, since prenatal ultrasound will have revealed the defect, doctors give medicines called prostaglandins, even before birth, to keep the ductus arteriosus from closing. Otherwise, it tends to close by two days after birth, which could be a death sentence for a child with tricuspid atresia.
In terms of surgical strategy, the natural question to ask is whether surgeons could open a passageway from the right atrium to the right ventricle and implant some kind of artificial tricuspid valve. But they cannot do this, because, during fetal life, the right ventricle atrophies. Its muscular layer thins out and weakens, since it’s not filling with any blood. Thus, in a newborn with tricuspid atresia, the right ventricle is not really useful as a pump. It’s useful initially just as a conduit for getting blood from the left ventricle to the pulmonary artery, so you’d have that, plus the ductus arteriosus — two pathways for blood to get into the pulmonary artery, so that it can travel through the lungs.
But the baby then needs to be transitioned into a kind of single ventricle physiology, since the right ventricle is basically useless as a pump. This transition happens with surgical procedures performed in a few stages, usually three stages. The first step typically is right after birth, when surgeons place what’s called a Blalock-Taussig shunt, a connection usually between the right subclavian artery (a large artery that branches off from the aorta) and right pulmonary artery. This shunt is doing the same thing as the ductus arteriosus, but it’s providing another pathway for blood from the aorta to reach the lungs.
The next stage is when the baby is about a year old, when surgeons perform what’s called a hemi-Fontan procedure. This establishes a route for some blood to move into the pulmonary artery, directly from the venous blood that’s headed to the right atrium from body tissues. Usually, the venous blood is routed from superior vena cava, the large vein that delivers blood from the head, neck, upper chest, and arms to the right atrium. Then, when the child is a few years old, the surgeons convert the shunting into what’s called a full Fontan by adding a shunt from the inferior vena vena cava (the big vein draining the lower body) to the pulmonary artery. There are various versions and modifications of the Fontan procedures, but the main idea is that you’re detouring around the right side of the heart, allowing the left ventricle to become the pump for one big circuit that includes the lungs, instead of having the right ventricle take care of that, since the right ventricle cannot handle the task anyway. It’s not as efficient as the two circuits being separate, each with a ventricle to pump it, but it can keep the child alive for many years, into adulthood, and during the intervening time new procedures and new devices will continue to emerge.