A lot of information, and also misinformation, regarding methods for extracting products of conception from the uterus have been circulating, particularly in the wake of the Supreme Court of the United States (SCOTUS) decision on the Dobbs versus Jackson Women’s Health Organization abortion case. This is the recent SCOTUS decision regarding a Mississippi law prohibiting abortions after 15 weeks gestation that ended up, not only upholding the Mississippi law, but also overturning the Roe V Wade decision of 1973. While prohibitions on abortion will be going into effect in many US states during the weeks and months to come, the enforcement of such rules may not be equal throughout each state. This makes it all the more important to discuss the various procedures used to end unwanted pregnancies, but also as treatment for pregnancies that end naturally.
The term procedural abortion means surgical abortions, in contrast with medical abortions, abortions that are achieved with medicines alone, without the need for instruments to be inserted into the uterus. There are a handful of such techniques and they are used, not only for elective termination of pregnancy (elective abortion), but also for cases in which pregnancy must be terminated to save the mother’s life and cases in which the pregnancy has ended, but products of conception remain within the uterus, where they also threaten the woman. Most OB/GYN residency programs do not require trainees to perform elective abortions. However, typically, the OB/GYNs who are most skilled and available to conduct medically necessary abortions and treatment of missed abortions (embryo or fetus is no longer viable, but has not been expelled from the uterus) and incomplete abortions (embryo or fetus is no longer viable, but has been only partially expelled) are the ones who did elect to learn how to perform elective abortions. With this perspective in mind, let’s discuss the different methods for extracting products of conception and the associated terminology, whether in elective procedures, or medically necessary procedures.
Before discussing the invasive procedures, we should note that the medical approach —administration of medication, usually the drugs mifepristone and misoprostol— is the best choice for most women, and today actually accounts for most abortions. But medical abortion has limitations, the main one being that it’s appropriate only during the early phase of pregnancy, generally up to 10 gestational weeks (10 weeks after the last menstrual period). Other contraindications include known allergies to the medications, ectopic pregnancy, bleeding disorders, being anemic (hemoglobin is below a certain level), and certain inherited problems of red blood cells). While bleeding also is an issue for surgical abortions, it’s generally easier to observe a surgical patient and control her bleeding, in contrast with a medical patient who may suffer severe bleeding at home. But don’t let these precautions worry you too much. Medical abortion is extremely safe in women overall, much safer than carrying any pregnancy to term. Certain other situations, such as having an intrauterine device, (IUD) and various health problems require a high level of caution.
In cases of ectopic pregnancy that does not abort on its own, obstetricians typically have to reach the pregnancy through the abdomen. Often this can be done by way of laparoscopic surgery in which a few tiny incisions are cut and the surgery is performed through tubes. When a pregnancy is located correctly in the endometrium of the uterus, however, but it goes bad or is unwanted, that’s when obstetricians can extract the products of conception through a vaginal route.
All of the vaginal methods begin with dilatation of the cervix, meaning the cervix is encouraged to open. This can be done with an instrument that the OB/GYN pushes through the cervix, typically after medication has been applied hours earlier to help the cervix to relax. Alternatively, the OB/GYN can insert what’s called a laminaria stick. This is made of seaweed and it expands as it absorbs water. After a few to several hours, the cervix can be open enough to allow a procedure. The dilatation is the “D” part of all the procedures.
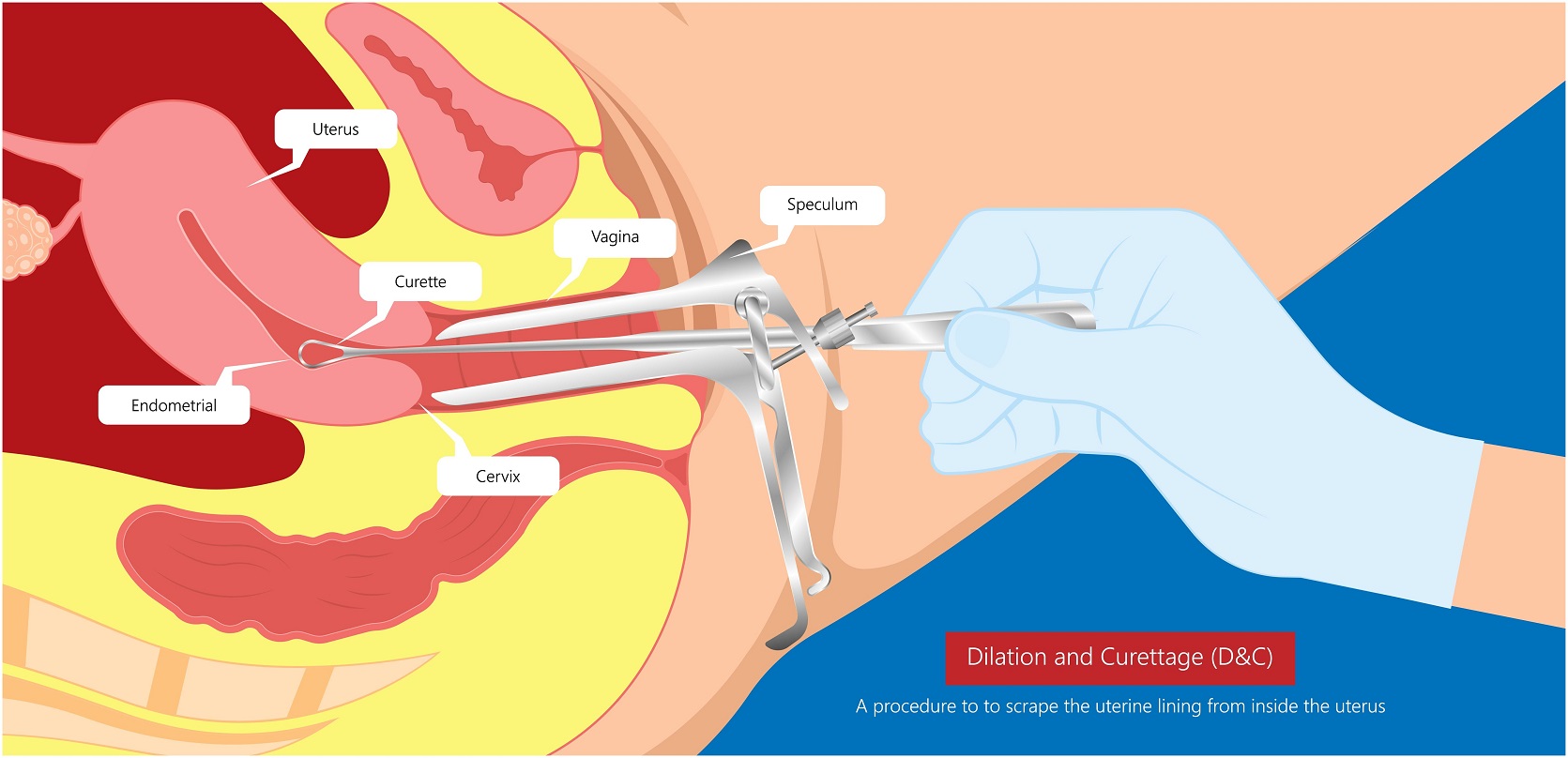
One such procedure is called a D&C, which stands for dilatation and curettage. Curettage is a kind of scraping of the inner lining of the uterus. Extracting a pregnancy, either viable or not, is only one of several reasons for performing a D&C. D&Cs can be performed for diagnostic reasons, such as when there’s a suspicion of abnormal cell growth in the endometrium. Therapeutic D&Cs can be performed for removing products of conception, but also for removing overgrowth of the uterine lining.
D&C by itself is adequate only early in pregnancy, so after a certain point the next option is dilatation and suction. This means that, after the cervix is dilated, the doctor suctions out the products of conception. Sometimes this can be done with a syringe, but often it requires power suction. A tube called a cannula is inserted through the opened cervix. Cannulae come in a range of sizes that are chosen based on how far along the pregnancy is, or was before it became inviable. In some cases, following suction, the doctor may then perform some curettage to extract any remaining products of conception.
At some point during pregnancy, generally around the midpoint, suction is not enough to extract either a viable or inviable fetus. In such cases, the OB/GYN must use instruments to grab onto the fetus, or parts of the fetus. Such a procedure is known as a D&E, which stands for dilatation and extraction. The extraction includes not only the fetus, but also the placenta, as well as the membranes. All the products of conception must be removed and accounted for, because products that remain inside the uterus can become infected. In discussing these techniques, notice how we have switched back and forth between mentioning elective and non-elective procedures. That’s because performing any of these procedures requires the same set of skills regardless of whether it’s a medical necessity, such as removal of retained products after a missed abortion, or it’s an unwanted pregnancy.