Continuing our discussion of congenital heart disease that began with Tetralogy of Fallot and transposition of the great arteries, let’s focus today on two more such conditions. One condition, called congenital pulmonary stenosis, or congenital pulmonic stenosis is somewhat common, especially in mild form and can be either acyanotic (not causing the baby to turn blue) or cyanotic, depending on how severe it is. Stenosis means narrowing and we’re talking about the pulmonary valve, the valve through which blood normally moves from the heart’s right ventricle into the pulmonary artery that carries blood to the lungs.
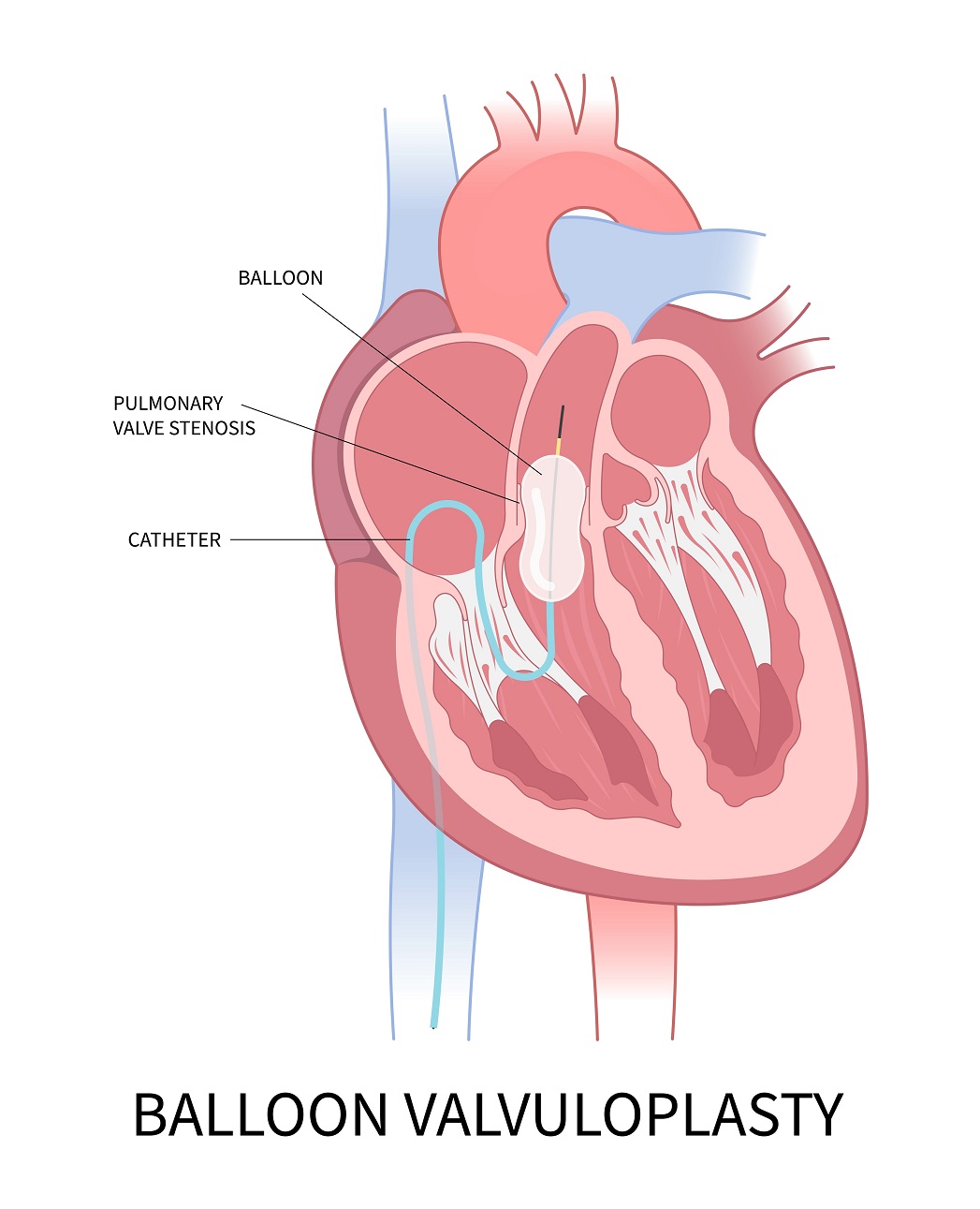
When the pulmonary valve is severely stenotic, severely narrowed, not much blood gets to into the pulmonary artery and through the lungs. If there’s no defect in the wall of the heart, no hole, pressure in the right ventricle is high, making pressure also high in the right atrium. This keeps the foramen ovale open after birth, because the way that the foramen ovale closes is with a flap, like a swinging door that swings into the left atrium. In fetal life, the foramen ovale is open constantly, allowing blood to move easily from the right atrium to the left atrium. Only if the pressure is a lot higher in the left atrium than the right atrium does the flap swing back against the interatrial septum, the wall separating the two atria. Normally this happens after birth. In cases of pulmonary stenosis, there also can be a defect in the wall that separates the two atria, the atrial septum, or there can be a defect in the wall that divides the two ventricles. If the pulmonary valve is very narrow, a good amount of blood —blue blood— will take one of these open pathways directly to the left side of the heart. This causes cyanosis, meaning that the baby looks blue in the skin, lips, and nailbeds. The main way to diagnose this condition is with echocardiography, an ultrasound of the heart. To treat congenital pulmonary stenosis, doctors use a catheter, a tube that goes through a major vein like the femoral vein in the leg. They navigate into the right ventricle and push open the valve with a balloon. This is called balloon valvuloplasty.
Another cyanotic congenital heart condition is truncus arteriosus, which is one big vessel carrying blood from the ventricles, instead of two, the aorta and pulmonary artery, but that one big vessel then splits into the aorta and pulmonary artery. That one big vessel, the truncus arteriosus, sits on top of a very defective wall that is supposed to separate the two ventricles, but does not, because it has a big hole, a defect. Blood entering the truncus from the not fully divided ventricles passes through a valve called the truncal valve, which usually is not a good valve. The condition is also called persistent truncus arteriosus, because really it’s just the persistence of an earlier developmental stage of the cardiovascular system, when the heart had just one ventricle, pumping into just one artery. As with tetralogy of Fallot, maternal diabetes —pregestational, not gestational— also raises the risk. Another risk factor is a condition called DiGeorge syndrome in which the long arm of chromosome 22 is missing. A third of all cases of truncus arteriosus are in DiGeorge syndrome babies.
So what happens in babies born with truncus arteriosus. First, the ventricular wall defect causes a lot of mixing of blood that enters the truncus and, initially, after birth, more than half of the blood takes the pulmonary artery route, rather than the aortic route, because of the lower pressure in the pulmonary vasculature. This high amount of pulmonary circulation has two main effects: The blood picks up a lot of oxygen and off-gases a lot of carbon dioxide, which is good. But the flip side is that the excessive pulmonary blood flow overloads the lungs. The higher-than-normal pulmonary blood flow can cause pulmonary edema (fluid in the lungs) and also pulmonary hypertension (high blood pressure in the lungs). This can lead to heart failure really quickly, even a week after birth, if there’s no intervention.
Management of truncus arteriosus depends on surgery that usually has to be performed within the weeks following birth, and it’s really complicated, since you’re starting with one big valve in the middle and have to end up with two valves, plus there’s a trunk that has to get divided or eliminated and remember that normally the coronary arteries emerge from the aorta at the aortic root. Surgeons need to know where they arise of the particular truncus architecture of the patient and decide what gets preserved and reshaped in what way and what pathway the coronary arteries will take in the new plan. So typically they’ll do cardiac catheterization —insert instruments through veins into the heart and take pictures of the arteries of the heart. This reveals the exact route of the coronary arteries and all of their branches. Meanwhile, there are some non-surgical therapies that can help the situation when doctors are waiting for the optimal time for surgery. Positive pressure ventilation, diuretic drugs (medicines that release water from the body), and medicines that squeeze blood out of the heart and get fluid out of the lungs.