Congenital heart disease occurs in about 1 percent of births and can take many forms. One such form, occurring in about 1 in every 3,000 births is Tetralogy of Fallot, which can have a variety of causes, some being things that you cannot control, such as history of the condition in your family, but others that are controllable risk factors. The latter category includes poor nutrition in pregnancy, consumption of alcohol while you are pregnant, and viral diseases during pregnancy that can be prevented through vaccination, notably rubella. Rubella is preventable by way of vaccination before you become pregnant. Although an incidence of 1 per 3,000 birth makes tetralogy a rare condition, it actually is the most common congenital cyanotic heart condition. This means a condition causing cyanosis, a deficiency of oxygen in body tissues causing the skin to appear bluish, or, in severe cyanosis, gray.
Malformations involving the heart or the great blood vessels attached to the heart cause cyanosis, if the condition causes blood to detour, or shunt, from the right side of the heart to the left side of the heart, or to the aorta (the large artery that carries blood from the heart’s left ventricle to the arteries that supply body tissues), without passing through the lungs. Normally, once a child is born, blood returning to the heart’s right atrium from body tissues moves through the right ventricle, the pulmonary artery to the lungs, from the lungs to the left atrium, through the left ventricle, and into the aorta to begin another trip through body tissues, but various conditions can cause shunts. A cyanotic shunt is a right-to-left shunt, because blood from body tissues does not get refreshed with oxygen, since it avoids the lungs, whereas a left-to-right shunt means that blood that has already passed through the lungs, so it is full of oxygen, detours to the right side of the circulation, instead of going directly to body tissues that need the oxygen and also need to get rid of carbon dioxide. Although not causing cyanosis, a left-to-right shunt can overload the right ventricle and the lungs with blood, which can be harmful, if the shunt is large, such that the ratio of blood volume passing through the lungs in a given amount of time compared with the blood volume passing through body tissues is high.
Although Tetralogy of Fallot is the most common congenital cyanotic heart condition, it is actually not the most common congenital heart condition causing cyanosis at birth. This is because many cases of tetralogy do not become cyanotic until later in infancy, or childhood, since there is a large variation of severity of the heart abnormalities of tetralogy. Instead, the most common congenital heart condition causing cyanosis at birth is an even more rare condition called transposition of the great arteries, meaning that the aorta receives blood from the right ventricle instead of the left, while the pulmonary artery receives blood from the left ventricle instead of the right. Since transposition means that the right and left blood circulations are not hooked up in series, but run in parallel —the left ventricle pumping blood around and around through body tissues, but not to the lungs, the right ventricle pumping blood through the lungs, only for it to return directly to the right side of the heart— the only reason why a newborn with transposition can stay alive is the presence of other connections, between the left and right blood. One such important connection is the ductus arteriosus, a blood vessel that connects the pulmonary artery and aorta during fetal life and which is still open at the moment of birth, but tends to close up by a month or so after birth. In babies with transposition, doctors will want to keep the ductus arteriosus open as long as possible (by giving the child chemicals called prostaglandins), until the child can have surgery, and the same is often true in cases of tetralogy. In some people, there also can be other connections between left and right blood.
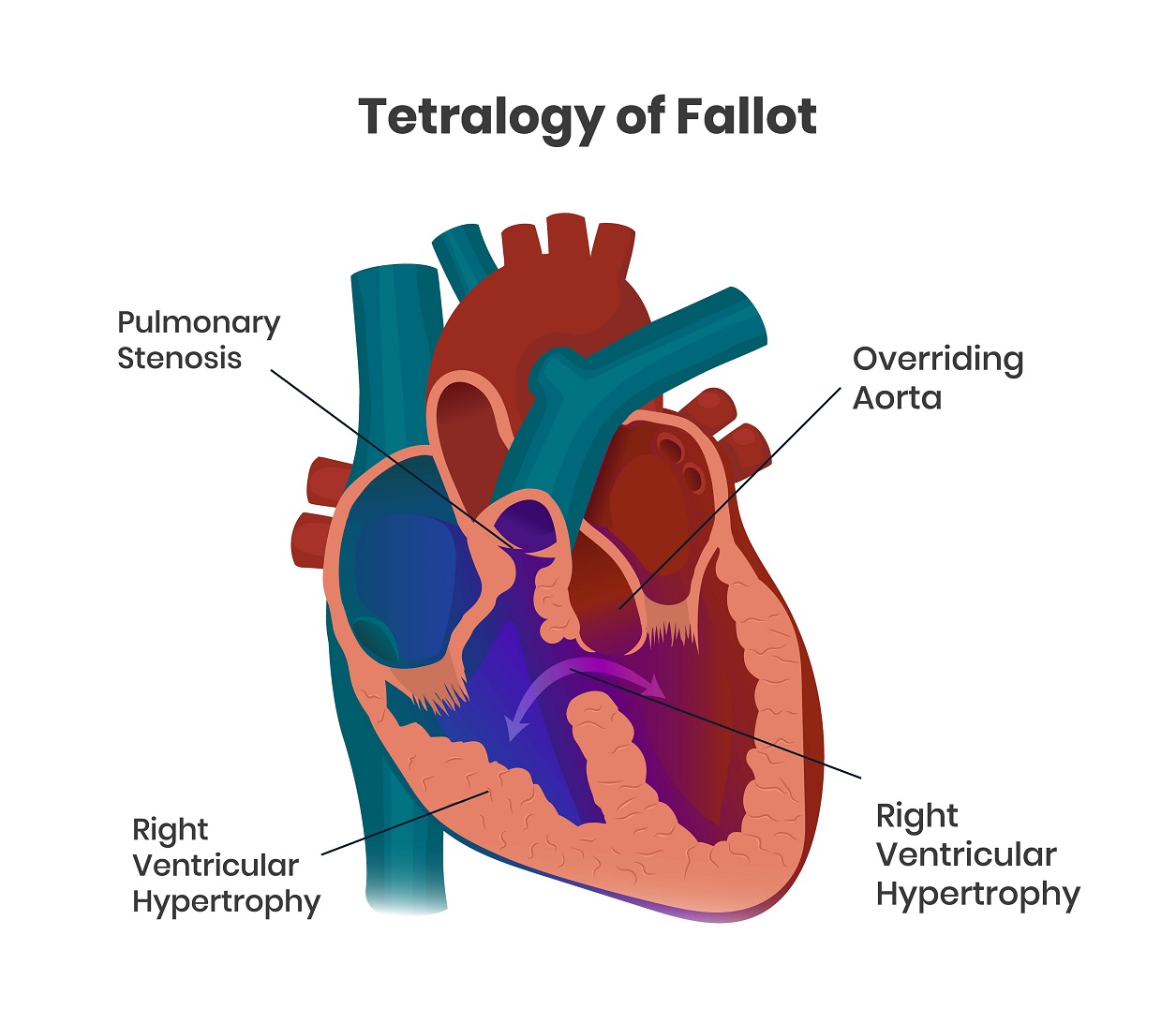
So what is tetralogy? From the Greek prefix tetra, you probably have an idea that tetralogy has something to do with the number four, which it does. First described in the late 19th century by Étienne-Louis Arthur Fallot, a French physician, tetralogy features four heart abnormalities. One of these is pulmonary stenosis, meaning that normal pathway from the right ventricle through the pulmonary artery is restricted; there isn’t enough room to get through, so blood is discouraged from going through the pulmonary artery and through the lungs. There also is a ventricular septal defect, meaning a hole between the two ventricles. The aorta, rather than emerging only from the left ventricle, overrides the right ventricle. Depending on how far shifted the aorta is to the right, varying amounts of blood from the right ventricle can enter the aorta, joining up with blood from the left ventricle that is entering the aorta as well. Finally, the muscular wall surrounding the right ventricle is hypertrophied, meaning it is too thick and strong, too much like how the left ventricular wall is supposed to be.
Though it may sound strange that four abnormalities should occur together as a particular condition, the name tetralogy is kind of a misnomer, because the four abnormalities are really all the result of just one problem. What happens in tetralogy is that something goes wrong with the formation of the intraventricular septum during embryonic and fetal life. The part of the developing intraventricular septum closer to the atrial end of the heart gets shifted toward the right, so it doesn’t align and link up with the part of the septum that’s developing from the direction of the heart’s apex. Shifting rightward, the malformed section of the septum, pulls the developing aorta rightward too, which is why the aorta ends up overriding the right ventricle, and also squeezes the outlet to the developing pulmonary artery, causing the pulmonary stenosis. The muscle surrounding the right ventricle hypertrophies, because in needs to pump against increasing pressure, due to the pulmonary stenosis and the aorta also receiving blood from the right ventricle. Furthermore, since the two ventricles end up with a connection between them, as pressure in the left ventricle increases at and after birth, the pressure increases further in the right ventricle. Essentially, the right ventricle has more of a burden than the left has, a burden that increases after birth, which is when the cyanosis can be absent or minimal at birth, but develop or worsen later.
So what is done for children who are born with tetralogy? It is corrected with surgery. Depending on the severity and specific features of each case, various procedures will be performed at various ages. Generally, what the surgeons will be doing, however is to open the pulmonary outflow (reduce or eliminate the pulmonary stenosis) and close the intraventricular septum.