As we discussed in the post about the circulatory system here on the Pulse, the aorta is the artery that carries blood from the heart’s left ventricle and branches into numerous arteries that carry blood through all body tissues. The aorta is therefore extremely critical. An aneurysm is a swelling of a blood vessel, a bulge, ballooning, or other distention that makes the blood vessel wider. This happens, due to the vessel wall being weak and stretched over time by the pressure of the blood. Although aneurysms can occur both in arteries and veins, venous aneurysms are very rare, while arterial aneurysms are quite common. An aortic aneurysm is an aneurysm that occurs in the aorta itself and this can happen in various regions of the aorta, so let’s take a tour through those regions.
Leaving the heart’s left ventricle, blood passes through the aortic valve, into the aorta itself. The attachment point between the valve and the beginning of the aorta is called the aortic root. From there, the aorta projects upward toward the head as the ascending aorta, then curves about 180 degrees to head toward the feet, and that curved part is called the aortic arch. From there, the aorta is straight and heads down, as what’s called he descending aorta, through the diaphragm, the muscle that helps you breathe and separates the thoracic cavity (chest cavity) from the abdominal cavity. Everything from the aortic root through the arch and the descending aorta until the diaphragm is together called the thoracic aorta. The rest of the aorta, which continues downward from the diaphragm is called the abdominal aorta.
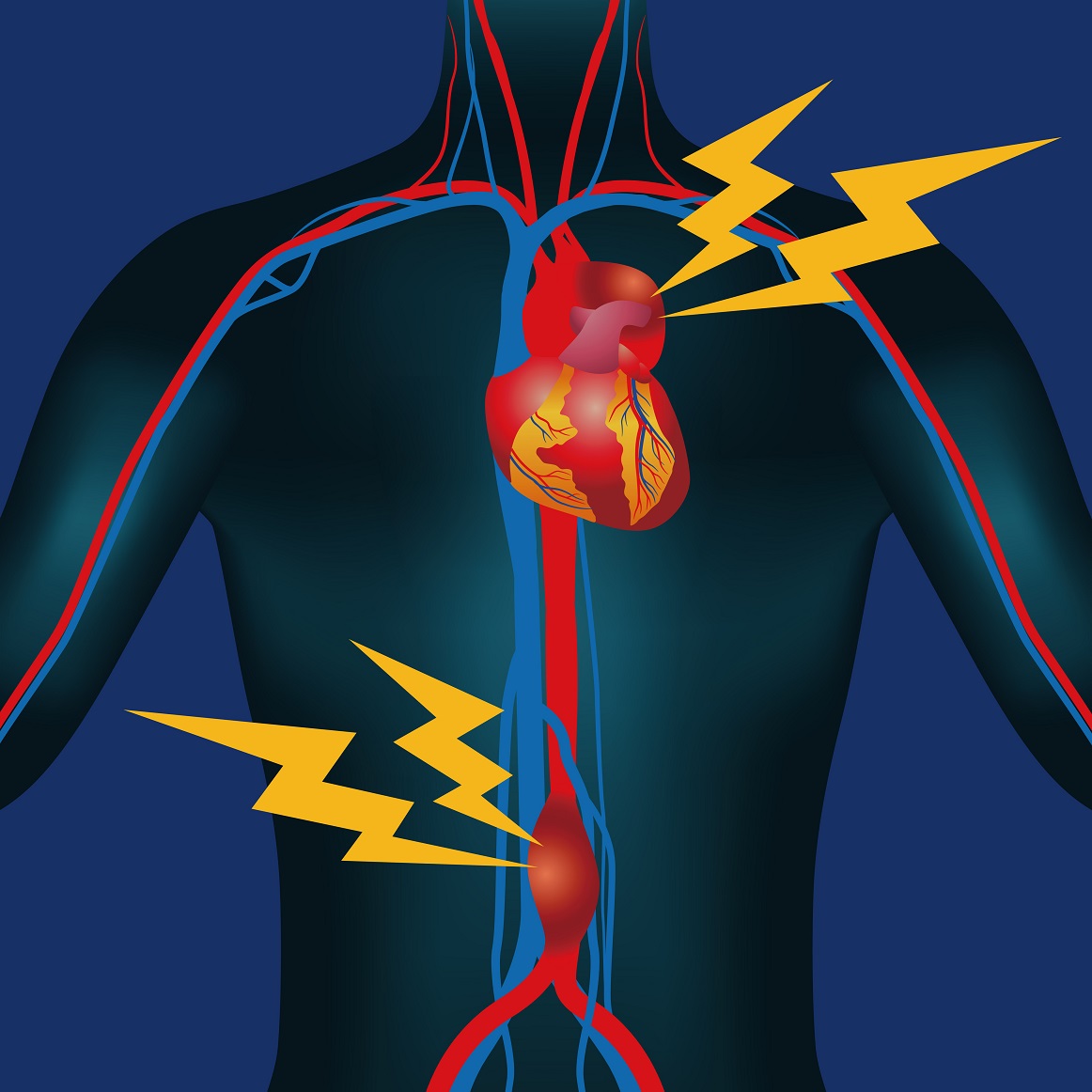
The main categories of aortic aneurysm are abdominal aortic aneurysm (AAA) and thoracic aortic aneurysm (TAA), plus it is possible to have mixtures of both types. An AAA is an aneurysm in the abdominal portion of the aorta. This means the part of the descending aorta downward from the diaphragm. TAA is an aneurysm anywhere in the thoracic aorta, which includes the ascending aorta (the portion of the aorta that extends upward from the aortic annulus that connects the aorta to the left ventricle), the aortic arch (the part that curves upward and then down), and the part of the descending aorta above the diaphragm (the descending thoracic aorta). Usually, with a TAA we’re talking about the ascending aorta and aortic arch. While AAA and TAA, as well as cerebral aneurysms, are fairly common, aneurysms also can occur in the wall of the heart itself and in arteries supplying organs, walls of body cavities, and limbs. In pregnancy, aneurysms have been discovered in arteries supplying the kidneys and spleen, although this is quite rare. It is difficult to estimate the actual prevalence of aortic aneurysm in pregnancy, because many such abnormalities are small and produce not symptoms, unless or until they grown.
Aneurysms are discovered, either when they produce symptoms, for instance if they are pushing on something, or if the body is being imaged for another reason. Factors that increase your risk of suffering an aortic aneurysm include high blood pressure, smoking, atherosclerosis, and certain genetic conditions of connective tissue, such as Ehlers-Danlos syndrome and Marfan syndrome.
However, with Marfan syndrome the main risk is not for a true aortic aneurysm. Rather, a special type called a dissecting aneurysm is part of a larger defect that also includes separation of the inner and middle layers of the artery wall. Such a separation is called aortic dissection.
TAA and AAA can be diagnosed with imaging procedures, such as ultrasound of the heart or abdomen, or computed tomography (CT) scanning or magnetic resonance imaging (MRI) of the chest or abdomen. CT of the abdomen is usually avoided during pregnancy itself, because it exposes your womb to some ionizing radiation.
Most aneurysms go unnoticed but changes in the body, such as the changes that occur in pregnancy, may possibly cause a small aneurysm to grow, or otherwise change. Complications that can occur from aortic aneurysms include pushing on nearby structures, formation of blood clots, aortic dissection, and actual rupture of the aneurysm, causing hemorrhage. Both aortic dissection and rupture of an aortic aneurysm are potentially fatal conditions. This threatens the life of the fetus as well.
A lot of controversy surrounds the assessment of risk that an aneurysm will rupture. High blood pressure, smoking, presence of daughter aneurysms (an aneurysm balloons out from another aneurysm), and various other features of aneurysm shape are thought to increase the risk. An aortic aneurysm is considered to be present, if the diameter of the aorta is more than 3mm. Risk increases as the size of the aneurysm increases.
Management of an an aortic aneurysm includes surveillance with ultrasound and other imaging, often every few months. This helps doctors determine if the size of the aneurysm is stable, or if it is getting larger. Additionally, medications are given to lower blood pressure, which is likely to prevent the aneurysm from growing, or at least to minimize growth. Of the various blood pressure medications, the main ones useful during pregnancy, because of their pregnancy safety, are called beta blockers.
If an aortic aneurysm reaches a certain size, surgery becomes necessary to prevent rupture. If you are being monitored with imaging every few months, generally doctors will know in advance that surgery will be needed. Having such a condition is a good reason to plan your pregnancy, however, to avoid a scenario in which an aneurysm enlarges faster than expected and requires surgery during pregnancy (a very rare scenario).