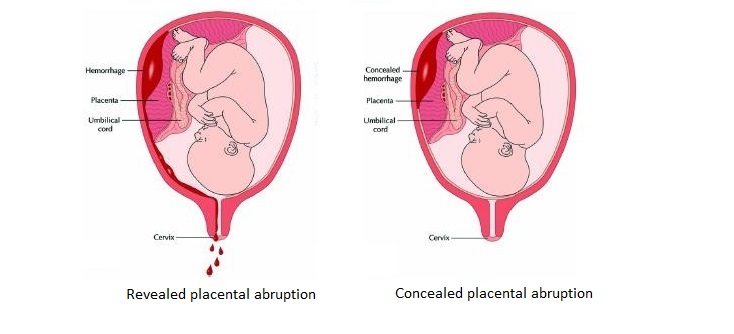
Types of abruption: A. With revealed abruption, blood tracks between the membranes and escapes through the vagina and cervix. B: With concealed abruption, blood collects behind the placenta, with no evidence of vaginal bleeding. From: Oyelese and Anathe. Placental Abruption. Obstet Gynecol 2006;108:1005-1016. Illustration by John Yanson.
Placental abruption is a relatively uncommon but serious pregnancy complication of pregnancy, affecting around 6.2 of every 1,000 pregnancies. It usually occurs between the 28th and 40th week of gestation and less frequently in the later part of the second trimester (between the 20th and 28th weeks). When it occurs, placental abruption can be sudden.
Placental abruption occurs when the placenta peels away from the wall of the uterus, either partially or completely. This condition can deprive the baby of nutrients and oxygen and can lead to premature birth or even stillbirth. For the mother, it can result in life-threatening bleeding, shock due to blood loss, the need for a blood transfusion, blood clotting problems or failure of the kidney or other vital organs.
Causes
The cause of placental abruption is usually unknown but can include injury or trauma to the abdomen (for example, from a car accident) or the rapid loss of fluid in the amniotic sac.
Risk factors include:
- Previous placental abruption
- High blood pressure or preeclampsia
- Substance abuse
- Blood-clotting disorders
- Multiple pregnancy (when you are carrying twins, triplets or more)
- Excessive alcohol consumption
- Diabetes
- Short umbilical cord
- Any uterine infection
- Uterine fibroids
- Age greater than 35
Symptoms
Classic symptoms of placental abruption include:
- Abdominal pain
- Vaginal bleeding
- Back pain
- Uterine tenderness
- Rapid uterine contractions
- Abdominal cramping and pain
- Nausea and vomiting
- Restlessness
- Abnormally enlarged uterus
In around 20% of cases there may be no bleeding – this is called a concealed placental abruption (see image above). In a concealed abruption, blood gets trapped inside the uterus and is pooled behind the placenta. This type of placental abruption can only be diagnosed with ultrasound.
Diagnosis
As well as a physical diagnosis to assess uterine stiffness or tenderness, other diagnostic tests may be used. These include:
- Abdominal ultrasound
- Blood tests (including a complete blood count and platelet count)
- Fetal monitoring
- Pelvic exam
- Vaginal ultrasound
Treatment
Treatment for placental abruption generally depends on the following circumstances:
- Time of gestation
- Severity of the separation
- Location of the separation
If your pregnancy is too early for your baby to be born (this is usually considered to be before 34 weeks of pregnancy), if your baby’s heart rate seems normal, and if the abruption is mild, then you might be admitted to the hospital for close monitoring. You may even be able to go home if your baby’s condition is stable and the bleeding stops. In the event that early delivery become necessary, you may be given a drug to help your baby’s lung mature.
If your baby is close to being full term (generally after 34 weeks of pregnancy) and the abruption seems minimal, a closely monitored vaginal delivery may be possible. However, if the abruption gets worse or puts your health or your baby’s health in jeopardy, then you will need an emergency C-section.
Unfortunately, there is no treatment that can either stop the placenta from detaching or that can reattach it once it has detached.
Prevention
Unfortunately, there is not much you can do to directly prevent placental abruption. However, you can lower your risk by quitting smoking and not using recreational drugs. If you have high blood pressure or preeclampsia, work with your healthcare provider to get it under control. If you have already experienced placental abruption with a previous pregnancy, discuss risk-reduction with your healthcare provider.